
SLIDE 1
6/25/2020 1 Unique Features
- f
Upper Extremity Muscle/Tendon Anatomy
Mark Elzik, MD Mission Viejo, CA
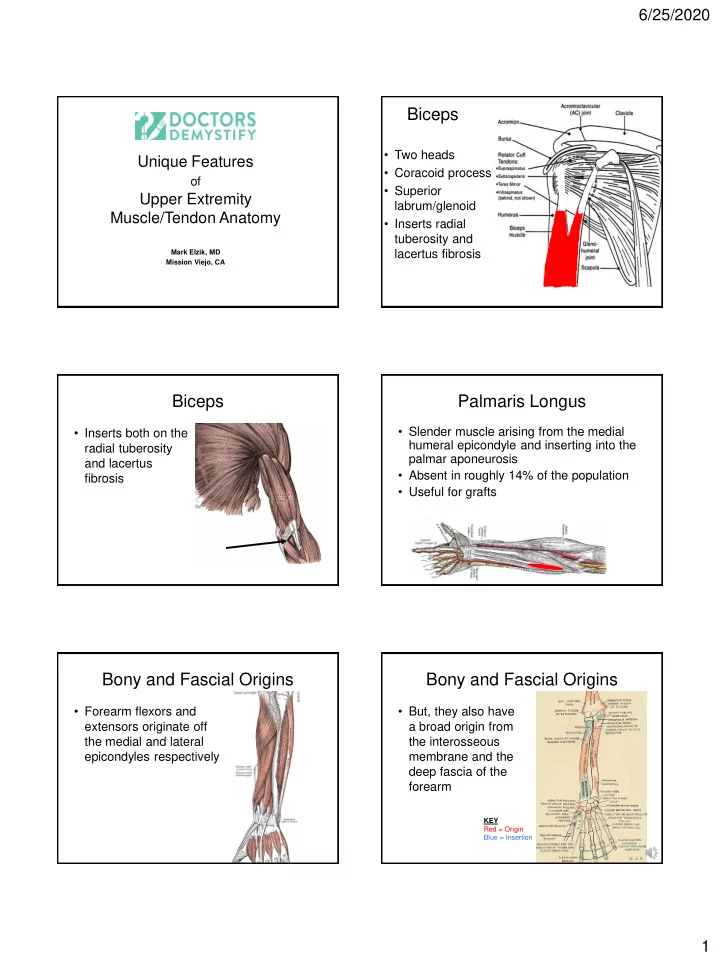
Biceps
- Two heads
- Coracoid process
- Superior
labrum/glenoid
- Inserts radial
tuberosity and lacertus fibrosis
Biceps
- Inserts both on the
radial tuberosity and lacertus fibrosis
Palmaris Longus
- Slender muscle arising from the medial
humeral epicondyle and inserting into the palmar aponeurosis
- Absent in roughly 14% of the population
- Useful for grafts
Bony and Fascial Origins
- Forearm flexors and
extensors originate off the medial and lateral epicondyles respectively
Bony and Fascial Origins
- But, they also have
a broad origin from the interosseous membrane and the deep fascia of the forearm
KEY Red = Origin Blue = Insertion