
9/30/2014 1
Practical Evaluation of the Adult with Intellectual/Developmental Disability and Suspected Dementia
- Julie A. Moran, D.O.
Consultant, Intellectual and Developmental Disabilities, Geriatrics, Tewksbury Hospital, Mass Dept. of Dev. Services Clinical Instructor of Medicine, Harvard Medical School
Background
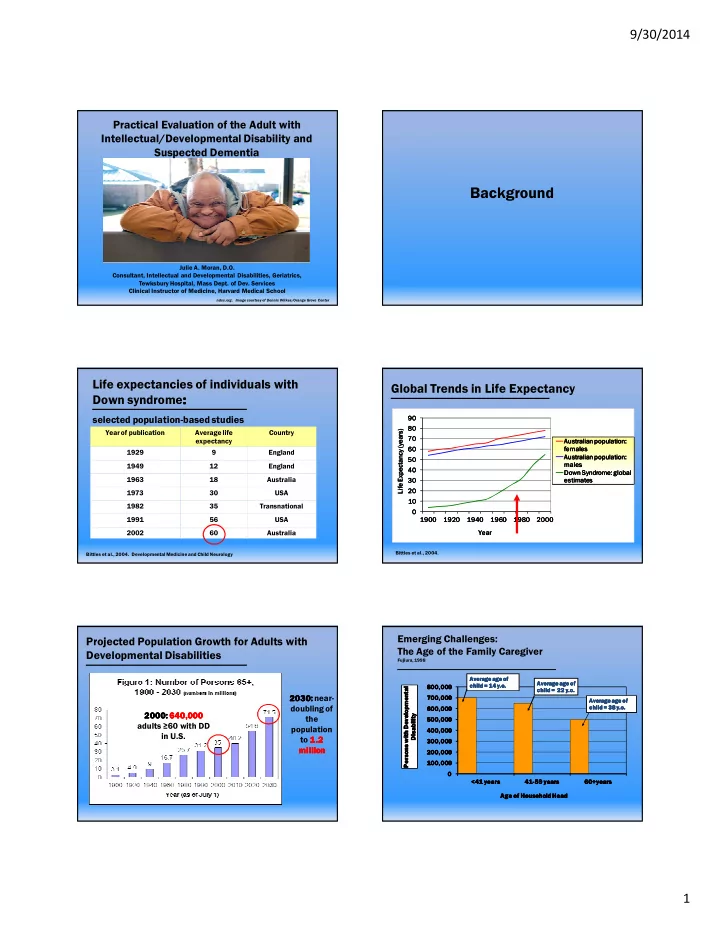
Year of publication Average life expectancy Country 1929 9 England 1949 12 England 1963 18 Australia 1973 30 USA 1982 35 Transnational 1991 56 USA 2002 60 Australia
Life expectancies of individuals with Down syndrome: : : :
selected population8based studies
Bittles et al., 2004. Developmental Medicine and Child Neurology
- !
! ! ! " " " " ! ! ! ! " " " " # $%& "!' ( # $%& "!' ( # $%& "!' ( # $%& "!' ( " " " "
Global Trends in Life Expectancy
Bittles et al., 2004
Projected Population Growth for Adults with Developmental Disabilities
2000 2000 2000 2000: : : : 640,000 640,000 640,000 640,000 adults ≥60 with DD in U.S. 2030 2030 2030 2030: : : : near8 doubling of the population to 1.2 1.2 1.2 1.2 million million million million
Emerging Challenges: The Age of the Family Caregiver
Fujiura, 1998
100,000 100,000 100,000 100,000 200,000 200,000 200,000 200,000 300,000 300,000 300,000 300,000 400,000 400,000 400,000 400,000 500,000 500,000 500,000 500,000 600,000 600,000 600,000 600,000 700,000 700,000 700,000 700,000 800,000 800,000 800,000 800,000 <41 years <41 years <41 years <41 years 41 41 41 418 8 8 859 years 59 years 59 years 59 years 60+years 60+years 60+years 60+years Persons with Developmental Persons with Developmental Persons with Developmental Persons with Developmental Disability Disability Disability Disability Age of Household Head Age of Household Head Age of Household Head Age of Household Head Average age of Average age of Average age of Average age of child = 22 child = 22 child = 22 child = 22 y.o y.o y.o y.o. . . . Average age of Average age of Average age of Average age of child = 38 child = 38 child = 38 child = 38 y.o y.o y.o y.o. . . . Average age of Average age of Average age of Average age of child = 14 child = 14 child = 14 child = 14 y.o y.o y.o y.o. . . .