
SLIDE 1
12/12/2015 1
Rotator Cuff or Rotator Cup: A rational approach to common shoulder problems
Brian Feeley, MD Associate Professor Department of Orthopaedic Surgery, University of California, San Francisco ABC Primary Care Sports Medicine 2015
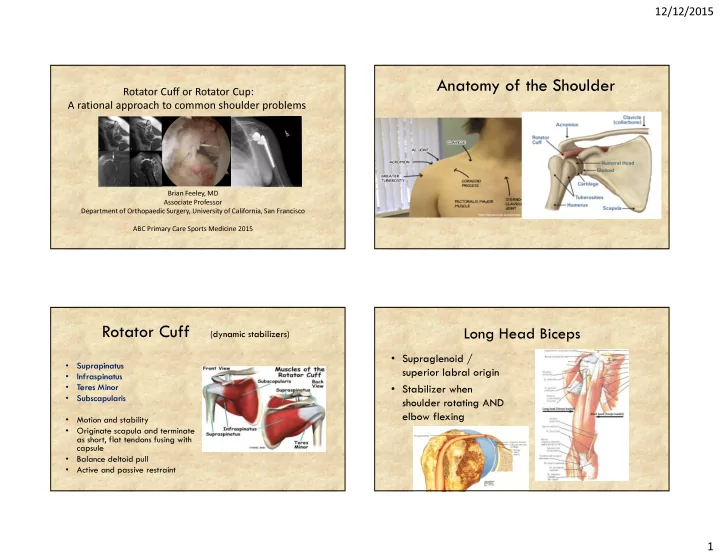
Anatomy of the Shoulder Rotator Cuff
(dynamic stabilizers)
- Suprapinatus
- Infraspinatus
- Teres Minor
- Subscapularis
- Motion and stability
- Originate scapula and terminate
as short, flat tendons fusing with capsule
- Balance deltoid pull
- Active and passive restraint
Long Head Biceps
- Supraglenoid /
superior labral origin
- Stabilizer when