
SLIDE 1
2/10/2017 1
Clinicopathologic Conference RAIN 2017
Case Presenter: Scott Caganap, MD Clinical Discussant: Gil Rabinovici, MD Pathology Discussant: Lea Grinberg, MD, PhD
Outline
- Case Presentation
- 1. History and Exam
- 2. Expert Opinion
- 3. Ancillary Testing
- 4. Final Diagnosis?
- Pathology Presentation
- Closing Remarks
Case Presentation
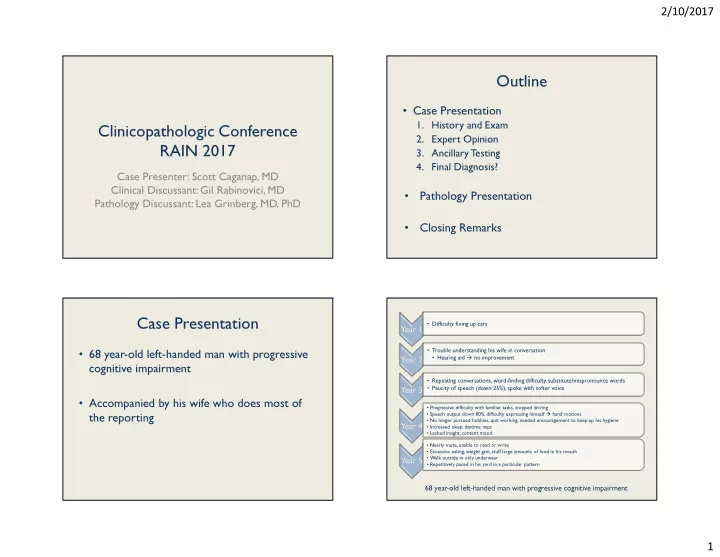
- 68 year-old left-handed man with progressive
cognitive impairment
- Accompanied by his wife who does most of
the reporting
Year 1
- Difficulty fixing up cars
Year 2
- Trouble understanding his wife in conversation
- Hearing aid no improvement
Year 3
- Repeating conversations, word-finding difficulty, substitute/mispronounce words
- Paucity of speech (down 25%), spoke with softer voice
Year 4
- Progressive difficulty with familiar tasks, stopped driving
- Speech output down 80%, difficulty expressing himself hand motions
- No longer pursued hobbies, quit working, needed encouragement to keep up his hygiene
- Increased sleep, daytime naps
- Lacked insight, content mood
Year 5
- Nearly mute, unable to read or write
- Excessive eating, weight gain, stuff large amounts of food in his mouth
- Walk outside in only underwear
- Repetitively paced in his yard in a particular pattern
68 year-old left-handed man with progressive cognitive impairment