
SLIDE 1
- - First shoulder arthroplasty
Reverse Total Shoulder Arthroplasty
James H. Chang May 3, 2007 UCSD
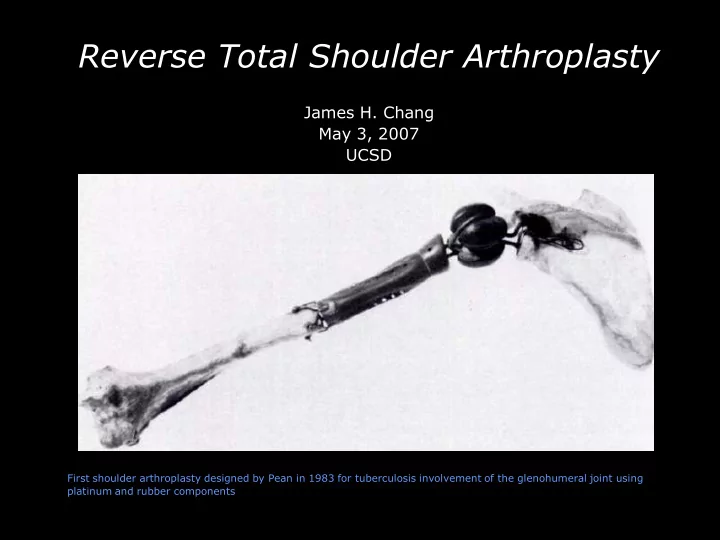
First shoulder arthroplasty designed by Pean in 1983 for tuberculosis involvement of the glenohumeral joint using platinum and rubber components