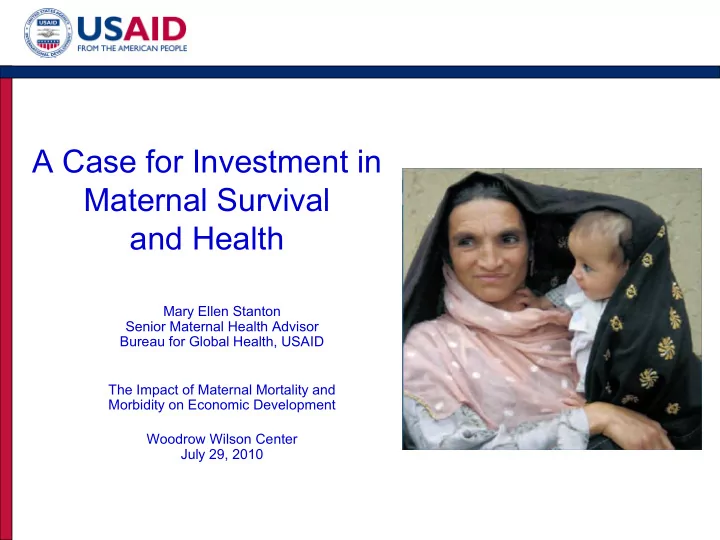
SLIDE 16 16.2 21.4 30.2 36.0 13.7 17.7 3.6 6.6 1.7 4.7 1.1 3.7 10 20 30 40 50 60 70 80 90 100 India * Indonesia Philippines Bangladesh Cambodia Nepal % of all births (bar height indicates total facility births) Private Govt NGO
The private sector is the site of a substantial and growing proportion of facility births
*India facility rates are for three years preceding the survey, because the 1998 data do not have information on births five years preceding survey. For all
- ther countries, these rates are for all births five years preceding survey. All DHS data; first time point was chosen to be from the fourth round of DHS
survey collection (1997-2003) while the second time point was chosen to be in the fifth phase (2003-Present).
Second Year First Year 33.6 40.8 14.6 9.9 11 46.1 37.9 44.2 39.7 21.5 9.1 17.7
Total Facility Births, by Facility Type, Asia, 1998—2008
M Koblinsky/JSI, S Alva/AIM, A Pomeroy/AIM