
SLIDE 1
4/24/2018 National Nursing Home Social Work Network - Webinar Series 1
Principal Investigator: Namkee Choi, PhD
Professor & Louis and Ann Wolens Centennial Chair in Gerontology
Community Partner: Meals on Wheels Central Texas
SOCIAL WORK LTSS RESEARCH AND POLICY NETWORK PRESENTATION
04/27/2018
Improving Access to Depression Treatment for Low-income Homebound Seniors Through Tele-delivered Counseling Presentation Order
- Late-life depression: Symptoms, DSM-5
criteria for major depressive disorder
- Etiology, stigma and misinformation, and
effects of untreated depression
- Evidence-based psychotherapy and access
barriers
- Research Projects 1, 2, and 3
- Challenges among low-income homebound
- lder adults
- Telehealth / telemental health policies
- Future of telemental health
Acknowledgment of Funding Sources for Research Projects 1-3
- National Institute of Mental Health (R34
MH083872)
- National Institute on Minority Health and
Health Disparities (1R01MD009675)
- AARP Foundation (national)
- St. David’s Foundation
- Mitte Foundation
- Almost everyone—
sometime in life
- Everyone knows someone
who suffers/suffered from depression.
- Even if you have never
been depressed, you can help someone if you have a better understanding of depression.
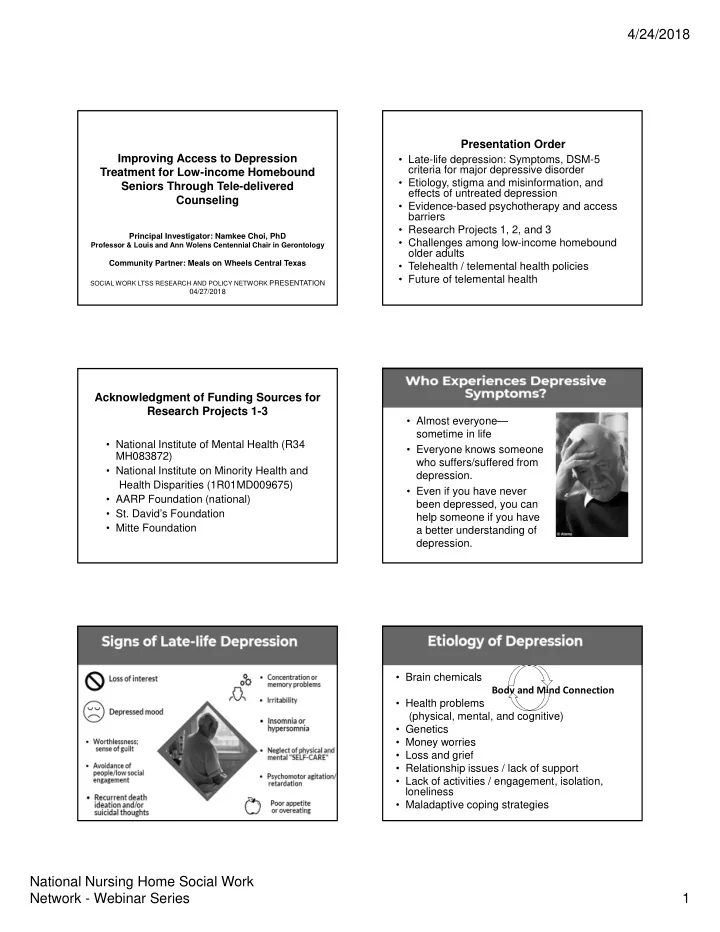
- Brain chemicals
Body and Mind Connection
- Health problems
(physical, mental, and cognitive)
- Genetics
- Money worries
- Loss and grief
- Relationship issues / lack of support
- Lack of activities / engagement, isolation,
loneliness
- Maladaptive coping strategies