
10/3/2016 1
J ES SIC A C O N KLIN , P HA R M D , P HC , B C A C P , A A HIV P , C D E V IS ITIN G A S S IS TA N T P R O FESSO R P HA R M A C Y P R A C TIC E A N D A D M IN ISTR A TIV E S C IEN C ES UN M C O LLEG E O F P HA R M A C Y J EC O N KLIN @ SA LUD . UN M . ED U
A PHARMACIST’S ROLE IN CARING FOR TRANSGENDER AND GENDER NON- CONFORMING PATIENTS
LEARNING OBJECTIVES
- De fine c urre nt a nd a ppro pria te vo c a b ula ry fo r
disc ussing tra nsg e nde r a nd g e nde r no n-c o nfo rming (T GNC) pe o ple .
- Re c o g nize b a rrie rs to he a lthc a re fa c e d b y T
GNC pe o ple
- Re c a ll c urre nt me dic a tio n the ra py o ptio ns fo r T
GNC pe o ple
- I
de ntify o ppo rtunitie s fo r pha rma c ist to pro vide po sitive , a ffirming c a re fo r T GNC pa tie nts
- L
ist re fe re nc e s tha t re info rc e a ppro pria te T GNC c a re
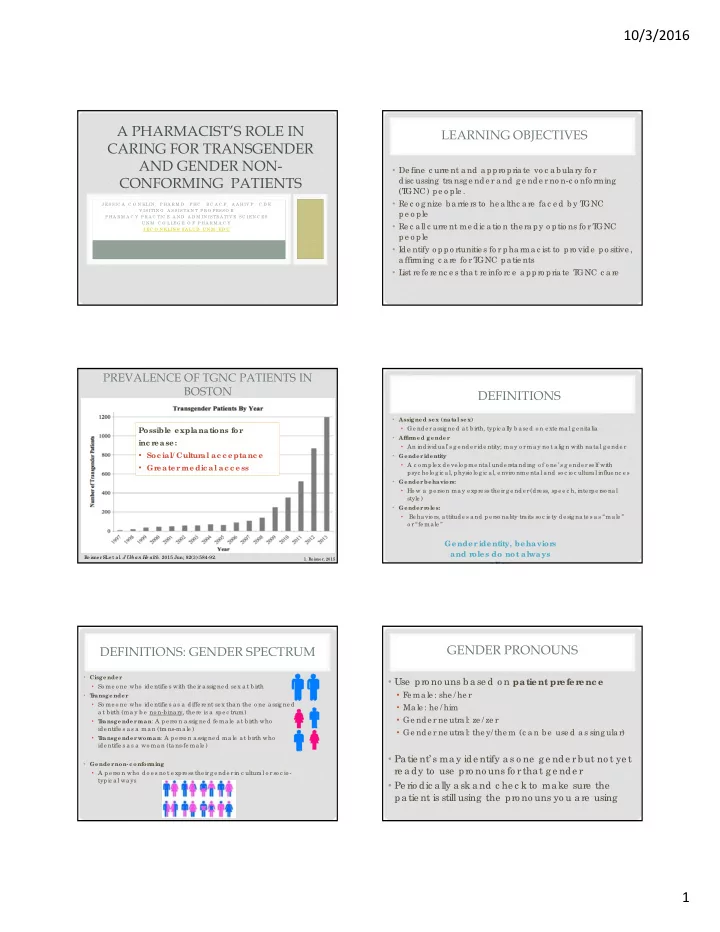
PREVALENCE OF TGNC PATIENTS IN BOSTON
- 1. Re isne r, 2015
Re isne rSL e t a l. J U rban He alth. 2015 Jun; 92(3):584-92.
Possible explanations for inc r ease:
- Soc ial/ Cultur
al ac c eptanc e
- Gr
eater medic al ac c ess
DEFINITIONS
- Assigne d se x (natal se x)
- Ge nde r a ssig ne d a t b irth, typic a lly b a se d o n e xte rna l g e nita lia
- Affir
me d ge nde r
- An individua l’ s g e nde r ide ntity; ma y o r ma y no t a lig n with na ta l g e nde r
- Ge nde r
ide ntity
- A c o mple x de ve lo pme nta l unde rsta nding o f o ne ’ s g e nde r se lf with
psyc ho lo g ic a l, physio lo g ic a l, e nviro nme nta l a nd so c io c ultura l influe nc e s
- Ge nde r
be havior s:
- Ho w a pe rso n ma y e xpre ss the ir g e nde r (dre ss, spe e c h, inte rpe rso na l
style )
- Ge nde r
r
- le s:
- Be ha vio rs, a ttitude s a nd pe rso na lity tra its so c ie ty de sig na te s a s “ma le ”
- r “fe ma le ”
Gender identity, behavior s and r
- les do not always
align
DEFINITIONS: GENDER SPECTRUM
- Cisge nde r
- So me o ne who ide ntifie s with the ir a ssig ne d se x a t b irth
- T
r ansge nde r
- So me o ne who ide ntifie s a s a diffe re nt se x tha n the o ne a ssig ne d
a t b irth (ma y b e no n-b ina ry, the re is a spe c trum)
- T
r ansge nde r man: A pe rso n a ssig ne d fe ma le a t b irth who ide ntifie s a s a ma n (tra ns-ma le )
- T
r ansge nde r woman: A pe rso n a ssig ne d ma le a t b irth who ide ntifie s a s a wo ma n (ta ns-fe ma le )
- Ge nde r
non-c onfor ming
- A pe rso n who do e s no t e xpre ss the ir g e nde r in c ultura l o r so c io -
typic a l wa ys
GENDER PRONOUNS
- Use pro no uns b a se d o n patient pr
efer enc e
- F
e ma le : she / he r
- Ma le : he / him
- Ge nde r ne utra l: ze / ze r
- Ge nde r ne utra l: the y/ the m (c a n b e use d a s sing ula r)
- Pa tie nt’ s ma y ide ntify a s o ne g e nde r b ut no t ye t
re a dy to use pro no uns fo r tha t g e nde r
- Pe rio dic a lly a sk a nd c he c k to ma ke sure the