
SLIDE 1
1
Squamous Cell Carcinoma of the Vulva and its Precursors
Charles Zaloudek, M.D. University of California, San Francisco
Squamous Cell Carcinoma
- Precursors
– Squamous intraepithelial lesions
- Mimics
– Herpes infection, Syphilis – Papillomatosis – Multinucleated Atypia
- Squamous cell carcinoma and variants
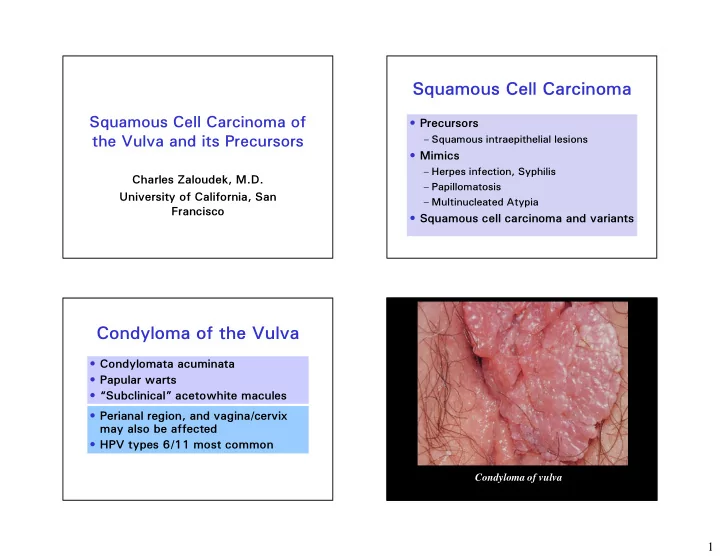
Condyloma of the Vulva
- Condylomata acuminata
- Papular warts
- “Subclinical” acetowhite macules
- Perianal region, and vagina/cervix
may also be affected
- HPV types 6/11 most common