
SLIDE 1
Smoking at Time of Delivery (SATOD)
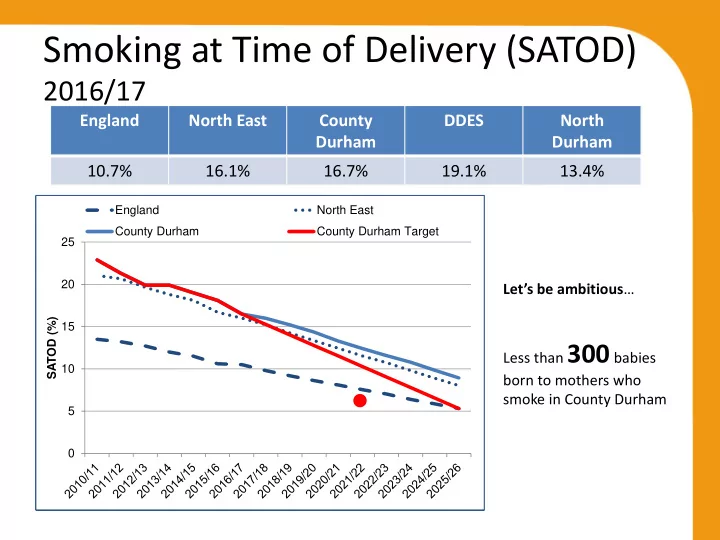
2016/17
England North East County Durham DDES North Durham 10.7% 16.1% 16.7% 19.1% 13.4%
5 10 15 20 25 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16 2016/17 SATOD (%) England North East County Durham 5 10 15 20 25 SATOD (%) England North East County Durham 5 10 15 20 25 SATOD (%) England North East County Durham 5 10 15 20 25 SATOD (%) England North East County Durham County Durham Target
2016/17
900 babies born to
mothers who smoke. If County Durham had the same % SATOD as England there would be around
340 less babies born to
smoking mothers. 2025/26
460 babies born to
mothers who smoke. If County Durham had the same % SATOD as England there would be around
180 less babies born to
smoking mothers. Let’s be ambitious… Less than 300 babies born to mothers who smoke in County Durham