
SLIDE 1
BIOL 6505 – Introduction to fetal medicine
Pulmonary Anomalies BIOL 6505 Introduction to fetal medicine - - PowerPoint PPT Presentation
Pulmonary Anomalies BIOL 6505 Introduction to fetal medicine Mammalian Airway Differentiation BIOL 6505 Introduction to fetal medicine Pulmonary Development Five stages From foregut to tracheal bud (embryonic phase)
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
Alveolarization ~36 wks 18 months Pseudoglandular stage 16-18 wks Saccular stage 26-36 wks
BIOL 6505 – Introduction to fetal medicine
cAMP PTHrP PTHrP-R TG uptake and release TG incorporation IGF-I, KGF,IL-6, IL-11
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
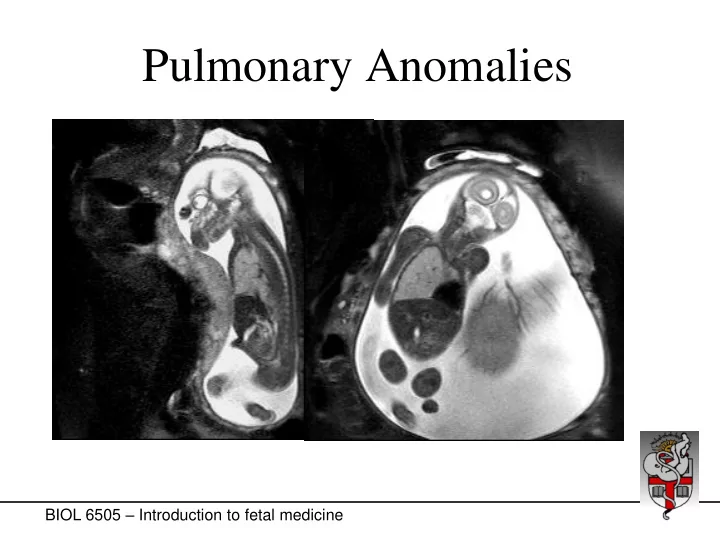
Chest wall Amniotic fluid Lungs Thoracic cavity
BIOL 6505 – Introduction to fetal medicine
Chest wall Amniotic fluid Lungs Thoracic cavity
BIOL 6505 – Introduction to fetal medicine
Chest wall Amniotic fluid Lungs Thoracic cavity
BIOL 6505 – Introduction to fetal medicine
Chest wall Amniotic fluid Lungs Thoracic cavity
BIOL 6505 – Introduction to fetal medicine
Chest wall Amniotic fluid Lungs Thoracic cavity
BIOL 6505 – Introduction to fetal medicine
Chest wall Amniotic fluid Lungs Thoracic cavity
BIOL 5720 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
Normal lung Sequestration
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine
BIOL 6505 – Introduction to fetal medicine