
SLIDE 1
Primary Care Programme Board Discussions – 18th May and 10th June
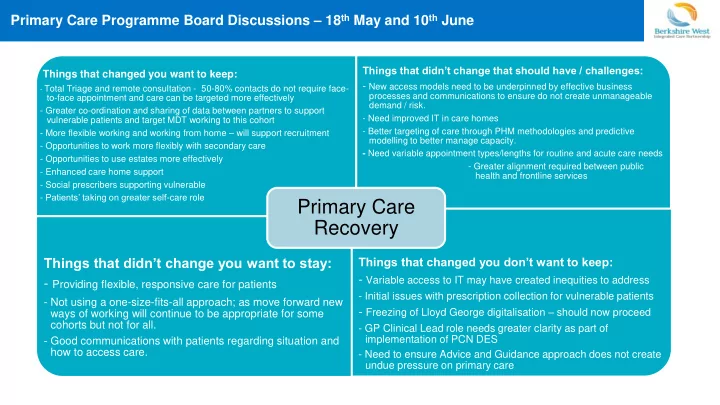
Things that changed you want to keep:
- Total Triage and remote consultation - 50-80% contacts do not require face-
to-face appointment and care can be targeted more effectively
- Greater co-ordination and sharing of data between partners to support
vulnerable patients and target MDT working to this cohort
- More flexible working and working from home – will support recruitment
- Opportunities to work more flexibly with secondary care
- Opportunities to use estates more effectively
- Enhanced care home support
- Social prescribers supporting vulnerable
- Patients’ taking on greater self-care role
Things that didn’t change that should have / challenges:
- New access models need to be underpinned by effective business
processes and communications to ensure do not create unmanageable demand / risk.
- Need improved IT in care homes
- Better targeting of care through PHM methodologies and predictive
modelling to better manage capacity.
- Need variable appointment types/lengths for routine and acute care needs
- Greater alignment required between public
health and frontline services
Things that didn’t change you want to stay:
- Providing flexible, responsive care for patients
- Not using a one-size-fits-all approach; as move forward new
ways of working will continue to be appropriate for some cohorts but not for all.
- Good communications with patients regarding situation and
how to access care.
Things that changed you don’t want to keep:
- Variable access to IT may have created inequities to address
- Initial issues with prescription collection for vulnerable patients
- Freezing of Lloyd George digitalisation – should now proceed
- GP Clinical Lead role needs greater clarity as part of
implementation of PCN DES
- Need to ensure Advice and Guidance approach does not create