
SLIDE 1
1
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice
Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Dislosures
- Clinical trial support from Genentech Inc.
Clinical Indicators of Increased Post- Operative Risk
- Tumor at or close to surgical margin
- Perineural Invasion
- Cartilage invasion
- Invasion of bone or soft tissues of the neck
- Emergent Tracheostomy
- Lymph-vascular Invasion
- Multiple (> 2) lymph node metastasis
- Extra capsular extension
Pre- Versus Post-operative Radiotherapy
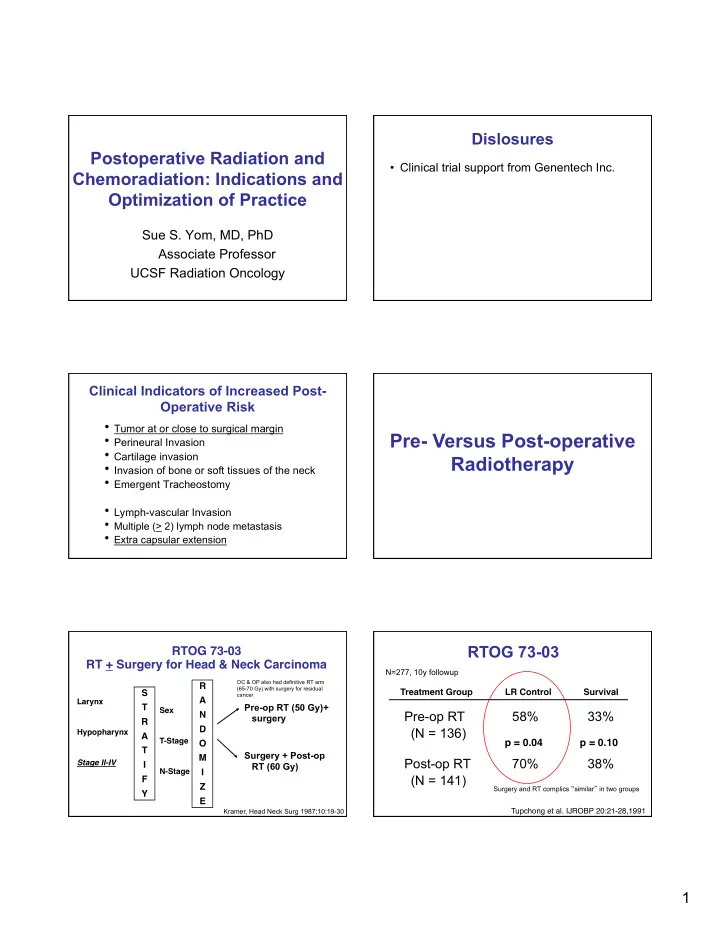
RTOG 73-03 RT + Surgery for Head & Neck Carcinoma
Larynx Hypopharynx Stage II-IV
S
- T
- R
- A
- T
- I
- F
- Y
- Sex
T-Stage N-Stage
R
- A
- N
- D
- O
- M
- I
- Z
- E
- Pre-op RT (50 Gy)+
surgery Surgery + Post-op RT (60 Gy)
Kramer, Head Neck Surg 1987;10:19-30
OC & OP also had definitive RT arm (65-70 Gy) with surgery for residual cancer
RTOG 73-03
Pre-op RT 58% 33% (N = 136) Post-op RT 70% 38% (N = 141)
p = 0.04
Treatment Group LR Control Survival
Tupchong et al. IJROBP 20:21-28,1991
p = 0.10
Surgery and RT complics “similar” in two groups
N=277, 10y followup