
SLIDE 1
Pediatric Artificial Lung (PAL)
Ronald B. Hirschl, M.D. Professor and Head, Pediatric Surgery Mott Children’s Hospital University of Michigan
No disclosures Work sponsored by NIH RO1-HD-015434
Pediatric Chronic Respiratory Failure
- CDH:
56% die or meet criteria for BPD at 30 days. The cost of CDH is $250 million annually Beyond age 4-5 years patients lead reasonably normal lives. Example: LTx in newborn with CDH and excised at 5 years.
- Hypoxemia, CO2 retention, and
pulmonary hypertension.
- CDH, BPD, ACD, interstitial lung
disease, and fibrosis following necrotizing pneumonia and ARDS.
DeAnda A , et al. J Ped Surg, 33:655, 1998
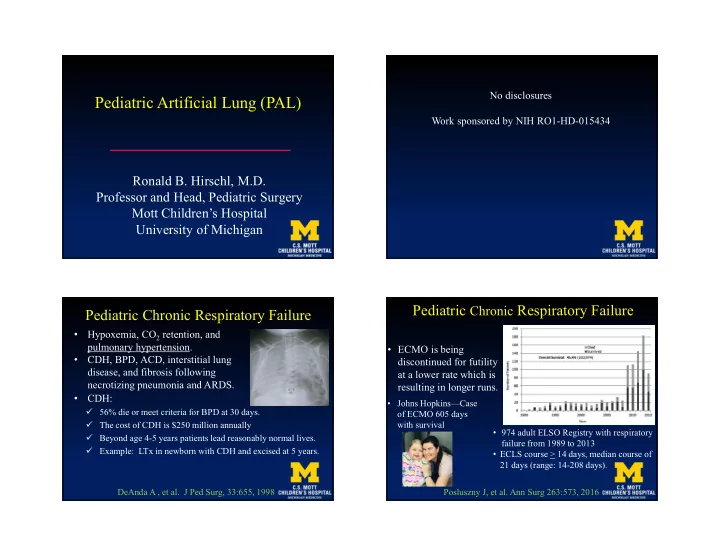
Pediatric Chronic Respiratory Failure
- ECMO is being
discontinued for futility at a lower rate which is resulting in longer runs.
Posluszny J, et al. Ann Surg 263:573, 2016
- Johns Hopkins—Case
- f ECMO 605 days
with survival
- 974 adult ELSO Registry with respiratory
failure from 1989 to 2013
- ECLS course > 14 days, median course of