
SLIDE 1
1
Pediatric Visual Pediatric Visual Dermatological Diagnosis Dermatological Diagnosis
Fernando Vega, M.D.
Objectives
- Recognize common pediatric
dermatologic conditions
- Expand differential diagnosis
Expand differential diagnosis
- Review treatment plans
- Identify skin manifestations of systemic
disease
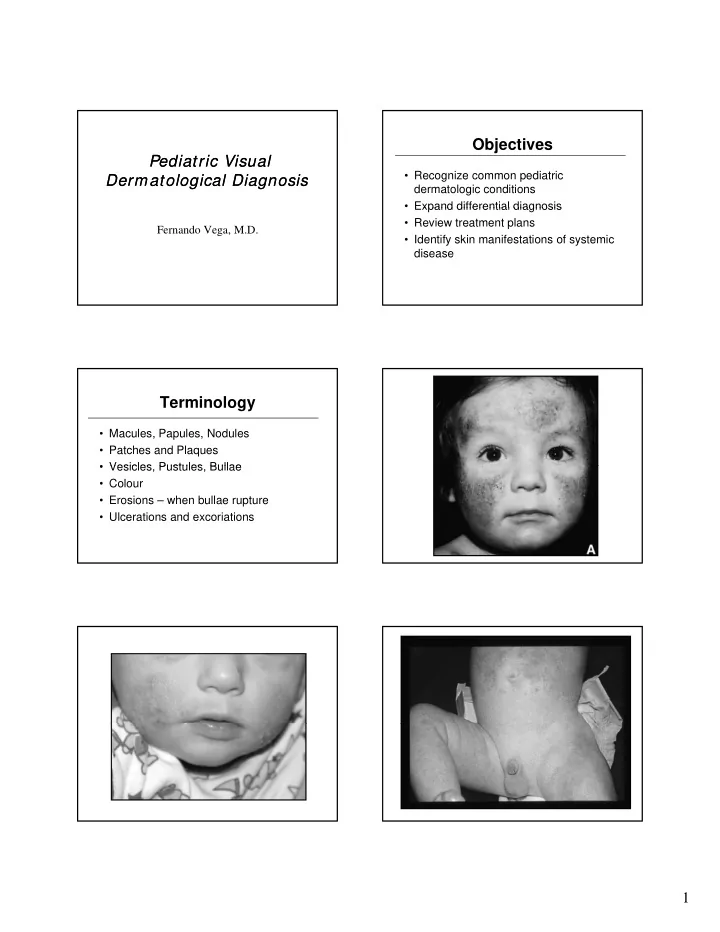
Terminology
- Macules, Papules, Nodules
- Patches and Plaques
- Vesicles Pustules Bullae
- Vesicles, Pustules, Bullae
- Colour
- Erosions – when bullae rupture
- Ulcerations and excoriations