
SLIDE 1
3/7/2015 1
The Postgraduate Course in Breast and Endocrine Surgery
Marines’ Memorial Club and Hotel San Francisco, CA Treatment of GI and Pancreatic Neuroendocrine Tumors
Eric K. Nakakura San Francisco, CA
March 6, 2015
GI and Pancreatic NETs
- Ipsen NET Advisory Board
Disclosures
Decision Tree
NET
Well- differentiated Well- differentiated
“carcinoid” “carcinoid” PNET PNET
Paraganglioma/pheochromocytoma Paraganglioma/pheochromocytoma
Poorly differentiated (high grade) Poorly differentiated (high grade)
Platinum- based chemotx Platinum- based chemotx
Neuroendocrine tumors (NETs)
GI and Pancreatic NETs
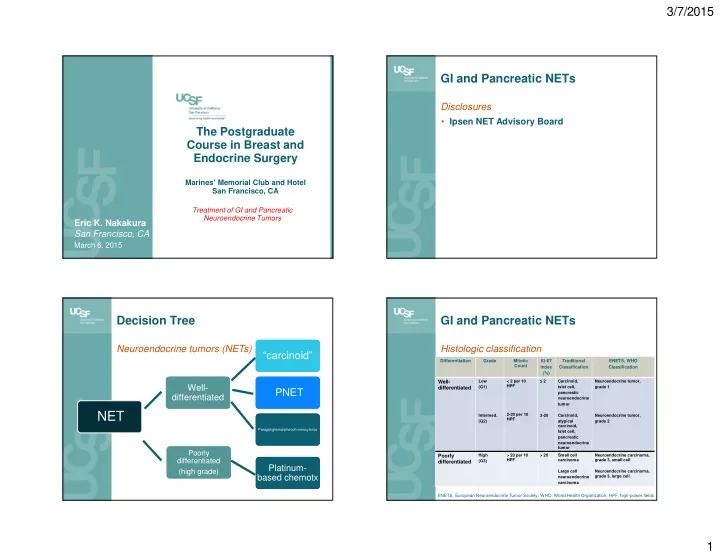
Histologic classification
Differentiation Grade Mitotic Count Ki-67 index (%) Traditional Classification ENETS, WHO Classification
Well- differentiated
Low (G1) Intermed. (G2) < 2 per 10 HPF 2-20 per 10 HPF ≤ 2 3-20 Carcinoid, islet cell, pancreatic neuroendocrine tumor Carcinoid, atypical carcinoid, Islet cell, pancreatic neuroendocrine tumor Neuroendocrine tumor, grade 1 Neuroendocrine tumor, grade 2
Poorly differentiated
High (G3) > 20 per 10 HPF > 20 Small cell carcinoma Large cell neuroendocrine carcinoma Neuroendocrine carcinoma, grade 3, small cell Neuroendocrine carcinoma, grade 3, large cell ENETS, European Neuroendocrine Tumor Society; WHO, World Health Organization; HPF, high-power fields