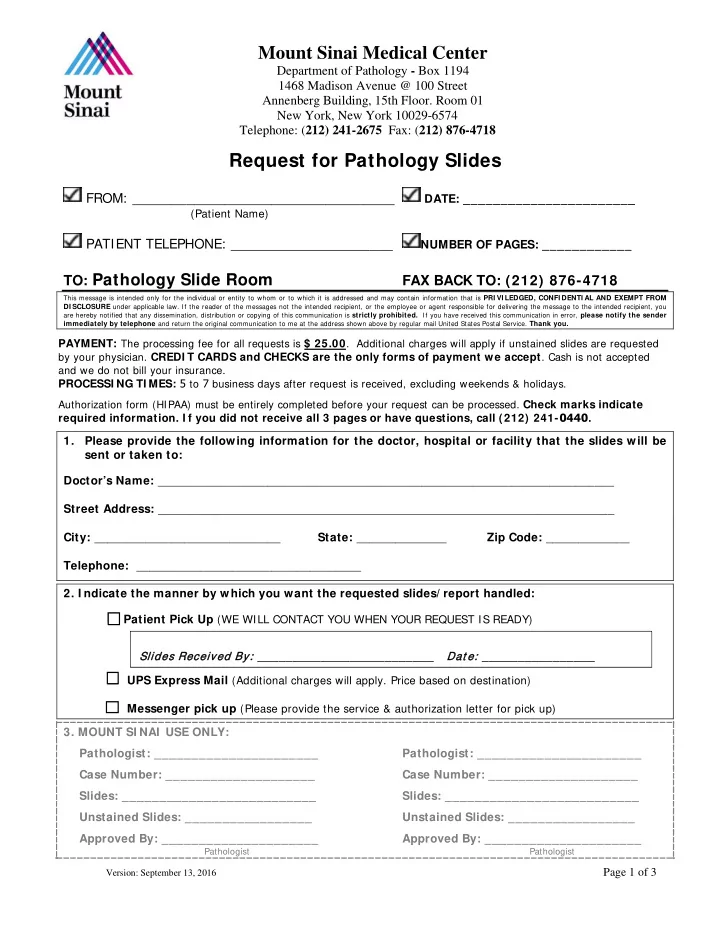

Request for Pathology Slides
FROM: __________________________________
DATE: _______________________ (Patient Name)
PATIENT TELEPHONE: _____________________
NUMBER OF PAGES: ____________
TO: Pathology Slide Room FAX BACK TO: (212) 876-4718
This message is intended only for the individual or entity to whom or to which it is addressed and may contain information that is PRI VI LEDGED, CONFI DENTI AL AND EXEMPT FROM DI SCLOSURE under applicable law. If the reader of the messages not the intended recipient, or the employee or agent responsible for delivering the message to the intended recipient, you are hereby notified that any dissemination, distribution or copying of this communication is strictly prohibited. If you have received this communication in error, please notify the sender immediately by telephone and return the original communication to me at the address shown above by regular mail United States Postal Service. Thank you.
PAYMENT: The processing fee for all requests is $ 25.00. Additional charges will apply if unstained slides are requested
by your physician. CREDI T CARDS and CHECKS are the only forms of payment we accept. Cash is not accepted and we do not bill your insurance.
PROCESSI NG TI MES: 5 to 7 business days after request is received, excluding weekends & holidays.
Authorization form (HIPAA) must be entirely completed before your request can be processed. Check marks indicate
required information. I f you did not receive all 3 pages or have questions, call (212) 241-0440. 1. Please provide the following information for the doctor, hospital or facility that the slides will be sent or taken to: Doctor’s Name: _______________________________________________________________________ Street Address: _______________________________________________________________________ City: _____________________________ State: ______________ Zip Code: _____________ Telephone: ___________________________________
- 2. I ndicate the manner by which you want the requested slides/ report handled:
□ Patient Pick Up (WE WILL CONTACT YOU WHEN YOUR REQUEST IS READY) □ UPS Express Mail (Additional charges will apply. Price based on destination) □ Messenger pick up (Please provide the service & authorization letter for pick up)
- 3. MOUNT SI NAI USE ONLY:
Pathologist: ______________________ Pathologist: ______________________ Case Number: ____________________ Case Number: ____________________ Slides: __________________________ Slides: __________________________ Unstained Slides: _________________ Unstained Slides: _________________ Approved By: _____________________ Approved By: _____________________
Pathologist Pathologist
Mount Sinai Medical Center
Department of Pathology - Box 1194 1468 Madison Avenue @ 100 Street Annenberg Building, 15th Floor. Room 01 New York, New York 10029-6574 Telephone: (212) 241-2675 Fax: (212) 876-4718
Slides es Rec ecei eived ed By: _________________________ Dat e: e: ________________
Version: September 13, 2016
Page 1 of 3