
SLIDE 1
7/13/2018 1
Mechanisms of Anabolic Therapy
John P. Bilezikian, MD, PhD (hon) Silberberg Professor of Medicine College of Physicians and Surgeons Columbia University New York, NY Osteoporosis CME 2018: New Insights in Research, Diagnosis, and Clinical Care July 12-13, 2018
John P. Bilezikian, MD, PhD (hon) Disclosures:
Abiogen (Consultant) Amgen (Consultant, Advisory Board) Shire Pharmaceuticals (Consultant) Radius Pharmaceuticals (Consultant, Advisory Board)
Regeneron (DSMB) Ultragenyx (Consultant)
6-18
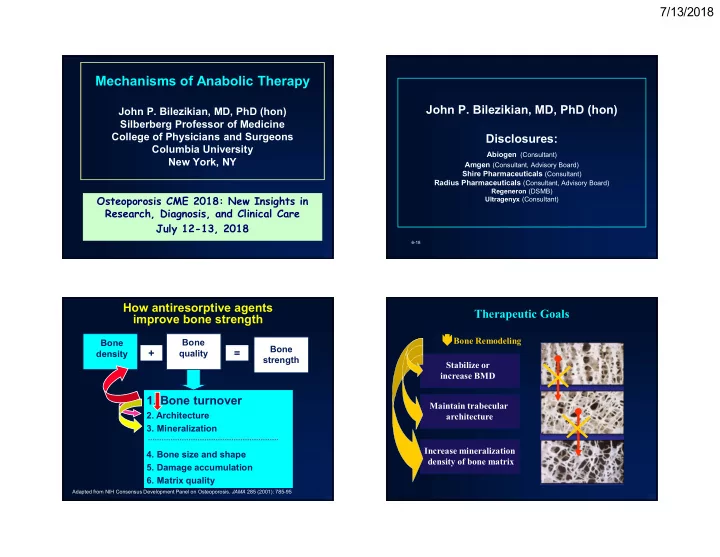
- 1. Bone turnover
- 2. Architecture
- 3. Mineralization
- 4. Bone size and shape
- 5. Damage accumulation
- 6. Matrix quality
+
Bone strength
How antiresorptive agents improve bone strength
=
Bone density Bone quality
Adapted from NIH Consensus Development Panel on Osteoporosis. JAMA 285 (2001): 785-95