
SLIDE 1
Introduction
- Recent growth in Health and Human Resources
spending has been dominated by Medicaid, which tends to dwarf all other program spending in HHR. − A one percent increase in Medicaid spending translates to $27 million in state funds.
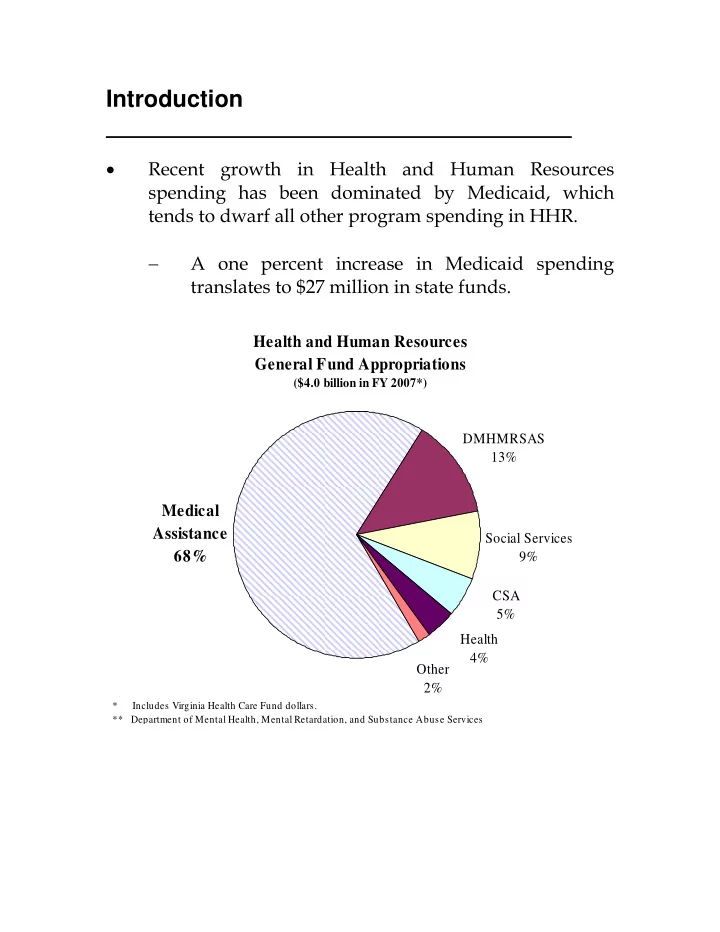
Health and Human Resources General Fund Appropriations
($4.0 billion in FY 2007*)
DMHMRSAS 13% Social Services 9% Other 2% Health 4% CSA 5%
Medical Assistance 68%
* Includes Virginia Health Care Fund dollars. ** Department of Mental Health, Mental Retardation, and Substance Abuse Services