
SLIDE 1
3/27/2013 1
INFECTIOUS DISEASES IN PEDIATRICS
Kevin Coulter MD Department of Pediatrics UC Davis Medical Center
Financial Disclosure
- I have no personal financial
relationship with a manufacturer of pharmaceutical products or services that will be discussed in this presentation.
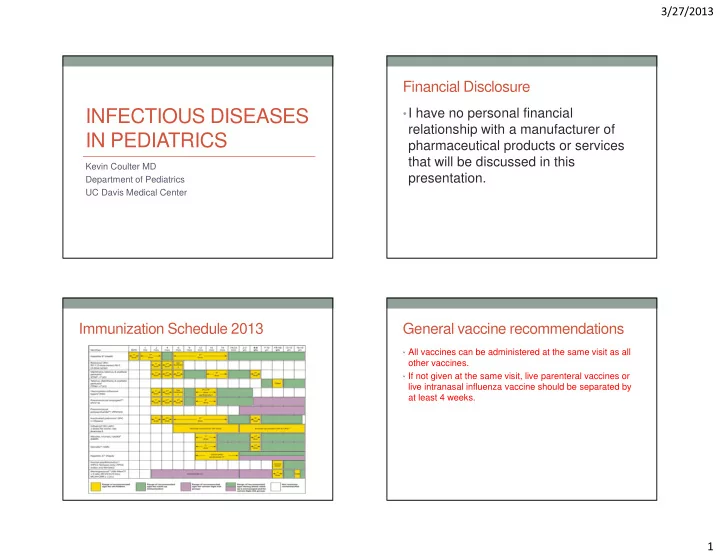
Immunization Schedule 2013 General vaccine recommendations
- All vaccines can be administered at the same visit as all
- ther vaccines.
- If not given at the same visit, live parenteral vaccines or
live intranasal influenza vaccine should be separated by at least 4 weeks.