
Rheumatologic Diseases Rheumatologic Diseases 6/23/2011 6/23/2011 Fernando Vega, M.D. Fernando Vega, M.D. 1
Rheumatological Rheumatological Diseases Diseases
Fernando Vega, MD Fernando Vega, MD HIHIM 409 HIHIM 409 July 2, 2009 July 2, 2009
Rheumatological Rheumatological Diseases Diseases
Disease Disease Autoantibody Autoantibody
Systemic Lupus Erythematosus Anti Systemic Lupus Erythematosus Anti-
- dsDNA, Anti
dsDNA, Anti-
- SM
SM Rheumatoid Arthritis Rheumatoid Arthritis RF, Anti RF, Anti-
- RA33
RA33 , Sjogrens Syndrome Sjogrens Syndrome Anti Anti-
- Ro(SS
Ro(SS-
- A),Anti
A),Anti-
- La(SS
La(SS-
- B)
B) Systemic Sclerosis Systemic Sclerosis Anti Anti-
- Scl
Scl-
- 70, Anti
70, Anti-
- centromere
centromere Polymyositis/Dermatomyositis Polymyositis/Dermatomyositis Anti Anti-
- Jo
Jo-
- 1
1 Mixed Connective Tissue Disease Anti Mixed Connective Tissue Disease Anti-
- U1
U1-
- RNP
RNP Wegener’s Granulomatosus Wegener’s Granulomatosus c c-
- ANCA
ANCA
Systemic Lupus Erythematosus Systemic Lupus Erythematosus
General
General
autoimmune multisystem disease
autoimmune multisystem disease
prevalence 1 in 2,000
prevalence 1 in 2,000
prevalence 1 in 2,000
prevalence 1 in 2,000
9 to 1; female to male (1 in 700)
9 to 1; female to male (1 in 700)
peak age 15
peak age 15-
- 25
25
immune complex
immune complex deposition deposition
Systemic Lupus Erythematosus Systemic Lupus Erythematosus
- Common complaints and presentations
Common complaints and presentations
Fever
Fever
Malaise
Malaise
Malaise
Malaise
Joint pains
Joint pains
Myalgias
Myalgias
Fatigue
Fatigue
Loss of cognitive abilities
Loss of cognitive abilities
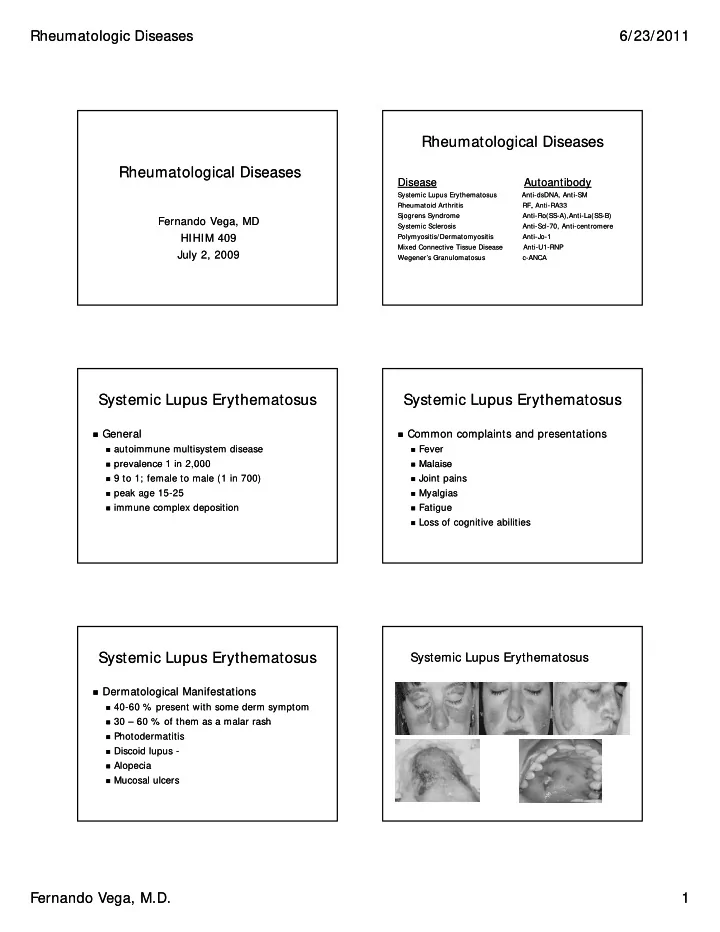
Systemic Lupus Erythematosus Systemic Lupus Erythematosus
Dermatological Manifestations
Dermatological Manifestations
40
40-
- 60 % present with some
60 % present with some derm derm symptom symptom
30
30 – 60 % of them as a 60 % of them as a malar malar rash rash
30
30 60 % of them as a 60 % of them as a malar malar rash rash
Photodermatitis
Photodermatitis
Discoid lupus
Discoid lupus -
- Alopecia
Alopecia
Mucosal ulcers