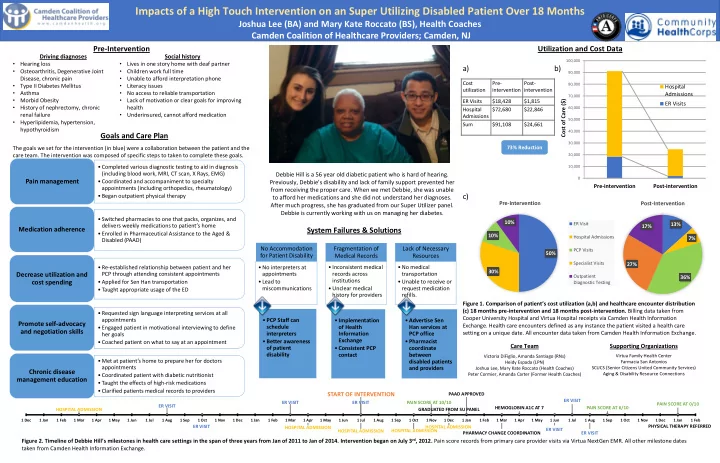

Utilization and Cost Data a) b) c)
Figure 1. Comparison of patient’s cost utilization (a,b) and healthcare encounter distribution (c) 18 months pre-intervention and 18 months post-intervention. Billing data taken from Cooper University Hospital and Virtua Hospital receipts via Camden Health Information
- Exchange. Health care encounters defined as any instance the patient visited a health care
setting on a unique date. All encounter data taken from Camden Health Information Exchange.
No Accommodation for Patient Disability
- No interpreters at
appointments
- Lead to
miscommunications
Fragmentation of Medical Records
- Inconsistent medical
records across institutions
- Unclear medical
history for providers
Lack of Necessary Resources
- No medical
transportation
- Unable to receive or
request medication refills.
.
Impacts of a High Touch Intervention on an Super Utilizing Disabled Patient Over 18 Months
Joshua Lee (BA) and Mary Kate Roccato (BS), Health Coaches Camden Coalition of Healthcare Providers; Camden, NJ
Debbie Hill is a 56 year old diabetic patient who is hard of hearing. Previously, Debbie’s disability and lack of family support prevented her from receiving the proper care. When we met Debbie, she was unable to afford her medications and she did not understand her diagnoses. After much progress, she has graduated from our Super Utilizer panel. Debbie is currently working with us on managing her diabetes.
Pre-Intervention
Driving diagnoses
- Hearing loss
- Osteoarthritis, Degenerative Joint
Disease, chronic pain
- Type II Diabetes Mellitus
- Asthma
- Morbid Obesity
- History of nephrectomy, chronic
renal failure
- Hyperlipidemia, hypertension,
hypothyroidism
Social history
- Lives in one story home with deaf partner
- Children work full time
- Unable to afford interpretation phone
- Literacy issues
- No access to reliable transportation
- Lack of motivation or clear goals for improving
health
- Underinsured, cannot afford medication
- Completed various diagnostic testing to aid in diagnosis
(including blood work, MRI, CT scan, X Rays, EMG)
- Coordinated and accompaniment to specialty
appointments (including orthopedics, rheumatology)
- Began outpatient physical therapy
Pain management
- Switched pharmacies to one that packs, organizes, and
delivers weekly medications to patient’s home
- Enrolled in Pharmaceutical Assistance to the Aged &
Disabled (PAAD)
Medication adherence
- Re-established relationship between patient and her
PCP through attending consistent appointments
- Applied for Sen Han transportation
- Taught appropriate usage of the ED
Decrease utilization and cost spending
- Requested sign language interpreting services at all
appointments
- Engaged patient in motivational interviewing to define
her goals
- Coached patient on what to say at an appointment
Promote self-advocacy and negotiation skills
- Met at patient’s home to prepare her for doctors
appointments
- Coordinated patient with diabetic nutritionist
- Taught the effects of high-risk medications
- Clarified patients medical records to providers
Chronic disease management education
Goals and Care Plan
The goals we set for the intervention (in blue) were a collaboration between the patient and the care team. The intervention was composed of specific steps to taken to complete these goals.
System Failures & Solutions
Care Team
Victoria DiFiglio, Amanda Santiago (RNs) Heidy Espada (LPN) Joshua Lee, Mary Kate Roccato (Health Coaches) Peter Cormier, Amanda Carter (Former Health Coaches)
10,000 20,000 30,000 40,000 50,000 60,000 70,000 80,000 90,000 100,000
Pre-intervention Post-intervention Cost of Care ($) Hospital Admissions ER Visits Figure 2. Timeline of Debbie Hill’s milestones in health care settings in the span of three years from Jan of 2011 to Jan of 2014. Intervention began on July 3rd, 2012. Pain score records from primary care provider visits via Virtua NextGen EMR. All other milestone dates taken from Camden Health Information Exchange.
HOSPITAL ADMISSION ER VISIT ER VISIT ER VISIT HOSPITAL ADMISSION HOSPITAL ADMISSION
START OF INTERVENTION
ER VISIT HOSPITAL ADMISSION PAIN SCORE AT 10/10 HOSPITAL ADMISSION GRADUATED FROM SU PANEL PAAD APPROVED PHARMACY CHANGE COORDINATION HEMOGLOBIN A1C AT 7 ER VISIT ER VISIT ER VISIT PAIN SCORE AT 6/10 PAIN SCORE AT 0/10 PHYSICAL THERAPY REFERRED
1 Dec 1 Jan 1 Feb 1 Mar 1 Apr 1 May 1 Jun 1 Jul 1 Aug 1 Sep 1 Oct 1 Nov 1 Dec 1 Jan 1 Feb 1 Mar 1 Apr 1 May 1 Jun 1 Jul 1 Aug 1 Sep 1 Oct 1 Nov 1 Dec 1 Jan 1 Feb 1 Mar 1 Apr 1 May 1 Jun 1 Jul 1 Aug 1 Sep 1 Oct 1 Nov 1 Dec 1 Jan 1 Feb
50% 30% 10% 10%
Pre-Intervention
ER Visit Hospital Admissions PCP Visits Specialist Visits Outpatient Diagnostic Testing
13% 7% 36% 27% 17%
Post-Intervention
- PCP Staff can
schedule interpreters
- Better awareness
- f patient
disability
- Implementation
- f Health
Information Exchange
- Consistent PCP
contact
- Advertise Sen
Han services at PCP office
- Pharmacist
coordinate between disabled patients and providers
Cost utilization Pre- intervention Post- intervention ER Visits $18,428 $1,815 Hospital Admissions $72,680 $22,846 Sum $91,108 $24,661 73% Reduction
Supporting Organizations
Virtua Family Health Center Farmacia San Antonios SCUCS (Senior Citizens United Community Services) Aging & Disability Resource Connections