
SLIDE 1
3/7/2017 1
Head and Neck Cancers
Session Chair: Sue S. Yom, MD PhD
Department of Radiation Oncology University of California San Francisco
Assi Assistant t t to Sess Session Chair Chair
- Christopher H. Chapman, MD MS – UCSF, Radiation Oncology Resident
Panel Membe nel Members
- Alain Algazi, MD
UCSF, Medical Oncology
- Beth Beadle, MD PhD
Stanford, Radiation Oncology
- A. Dimitrios Colevas, MD Stanford, Medical Oncology
- Patrick Ha, MD
UCSF, Head and Neck Oncologic Surgery
- Chris Holsinger, MD
Stanford, Head and Neck Oncologic Surgery
- Jed Katzel, MD
Kaiser Permanente, Medical Oncology
- Shyam Rao, MD PhD
UC Davis, Radiation Oncology
- Jonathan Reiss, MD MS
UC Davis, Medical Oncology
Case 1
45 year-old man, persistent sore throat Remote 10 pack-year smoking history, otherwise healthy Ph Physical Exam: ysical Exam:
- Right tonsillar fossa mass
- 2 palpable ipsilateral nodes, not fixed/matted
To Tonsil b biopsy p1 p16+ or 6+ orop
- pharynx SCC
SCC
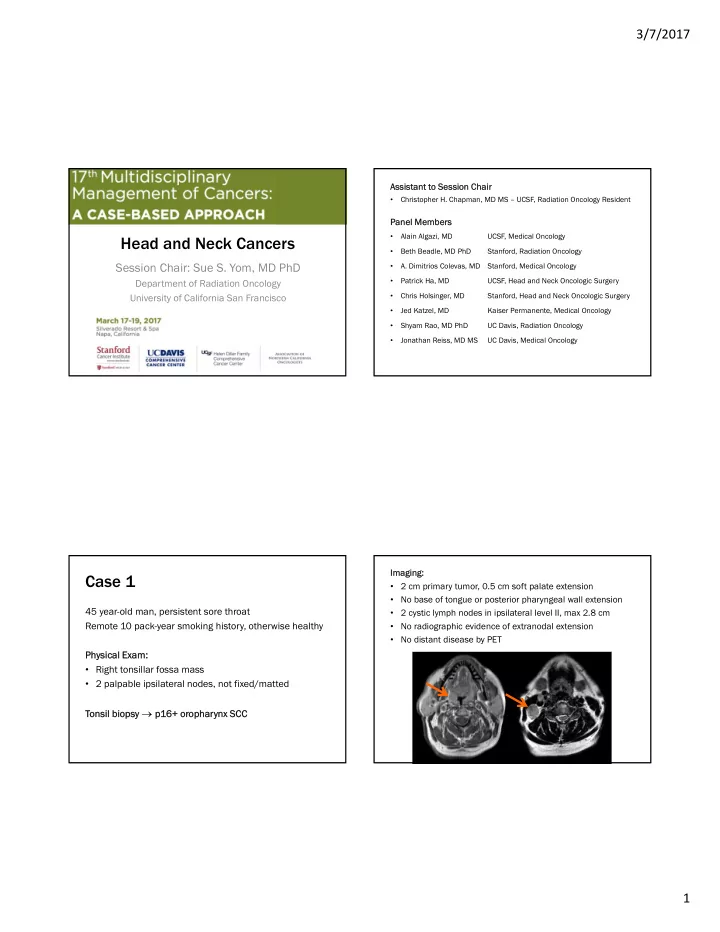
Imagi Imaging:
- 2 cm primary tumor, 0.5 cm soft palate extension
- No base of tongue or posterior pharyngeal wall extension
- 2 cystic lymph nodes in ipsilateral level II, max 2.8 cm
- No radiographic evidence of extranodal extension
- No distant disease by PET