
24/10/2013' 1'
Glomerulonephritis notes!
Notes to accompany online lectures at edrep.org/resources. They won’t make so much sense without seeing those. ! !
This work carries a Creative Commons Attribution-Noncommerical-Share Alike 2.5 UK: Scotland license. That means you may re-use it for non-commercial purposes as long as you clearly attribute it to us. For all other uses, contact us at renal@ed.ac.uk!
Neil Turner!
University of Edinburgh! www.edren.org www.edrep.org !
Glomerulonephritis 1 Neil Turner
Beth Shortt
Pre-renal
!
Heart failure! Shock !!
Systemic diseases !
Many and various:! Inflammatory/ immune! Metabolic! Other!
Collecting system and lower !
Congenital! Infection! Stones! Inflammation! Tumour!
Renal vasculature
!
Arterial stenosis! Venous thrombosis! Disease of arterioles!
Glomerular
!
Primary disease! Component of systemic disorder
!!
Interstitial
!
ATN (misnomer)! Toxic! Infective! Inflamm./ immune! Inherited!
Diseases of the urinary tract
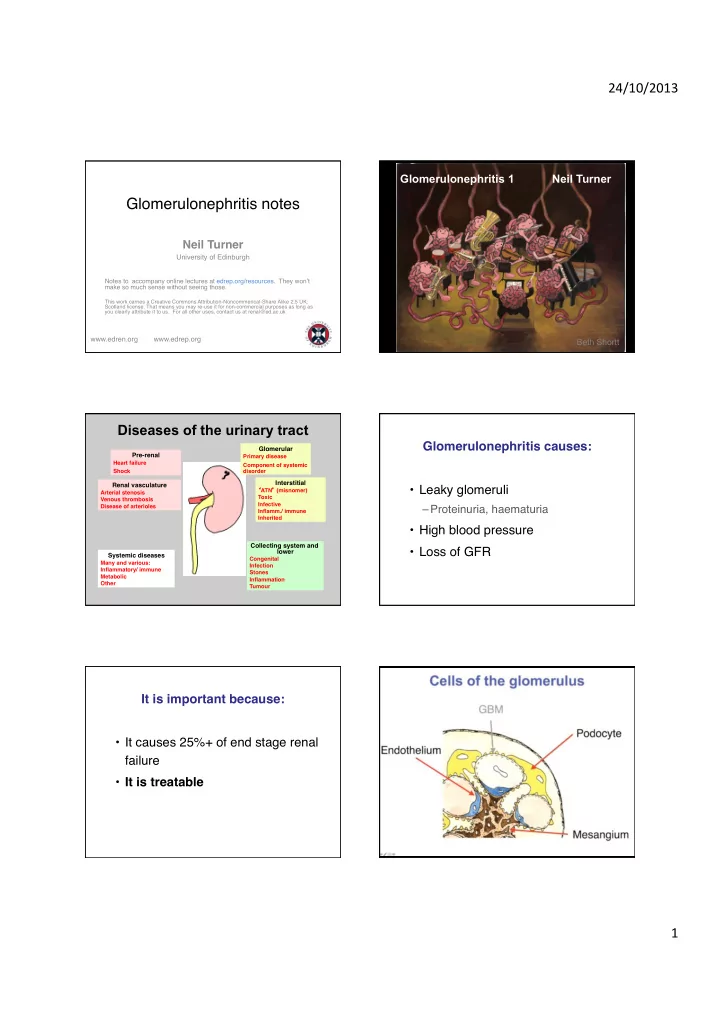
- Leaky glomeruli!
– Proteinuria, haematuria!
- High blood pressure!
- Loss of GFR!
Glomerulonephritis causes: !
- It causes 25%+ of end stage renal
failure!
- It is treatable!