
SLIDE 1
Genetics and Pregnancy Loss Dorothy Warburton Genetics and - - PDF document
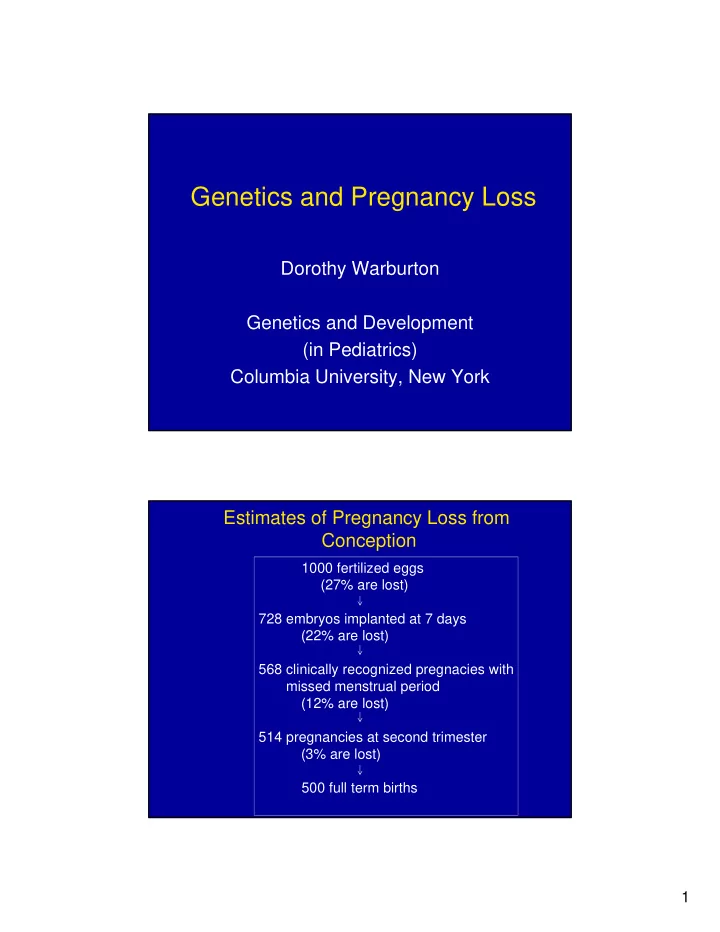
Genetics and Pregnancy Loss Dorothy Warburton Genetics and Development (in Pediatrics) Columbia University, New York Estimates of Pregnancy Loss from Conception 1000 fertilized eggs (27% are lost) 728 embryos implanted at 7 days (22% are
1000 728 568 514 500 100 200 300 400 500 600 700 800 900 1000 fertilized eggs implanted embryos recognized pregnancy 2nd trimester fetuses full term births
32% 46% 7% 12% 3% normal trisomy monosomy polyploid rearrangements
Frequency of Trisomy among Prenatal Diagnoses by Maternal Age
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48
Maternal Age
CVS Amniocentesis
10 20 30 40 50 60 70 19-22 23-26 27-30 31-34 35-38 39-42 43-46 Age Group
Adapted from (Pellestor, 2005)
10 20 30 40 50 60 20-24 25-29 30-34 35-39 40-44 45+
QuickTime™ and a TIFF (Uncompressed) decompressor are needed to see this picture.