
SLIDE 1
3/19/2015 1
FUNDAMENTALS OF OBSTETRICS
Christine Pecci, MD Department of Family and Community Medicine March 2015
- No disclosures
- Tanya is a 23 yo G1P0 who presents for early pregnancy
- care. This is a planned pregnancy and she has a sure
LMP that dates her to be 10 1/7 weeks EGA
- She had some bleeding yesterday and went to ED where
she had an US that puts her at 9 2/7 weeks (6 days different than EDD based on LMP)
- Reports regular menses q month
- Should you change her dating based on 1st trimester US?
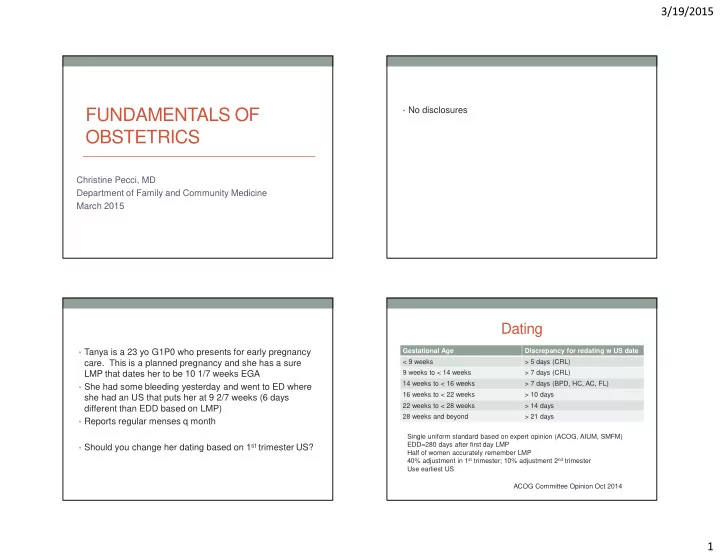
Dating
Gestational Age Discrepancy for redating w US date < 9 weeks > 5 days (CRL) 9 weeks to < 14 weeks > 7 days (CRL) 14 weeks to < 16 weeks > 7 days (BPD, HC, AC, FL) 16 weeks to < 22 weeks > 10 days 22 weeks to < 28 weeks > 14 days 28 weeks and beyond > 21 days ACOG Committee Opinion Oct 2014 Single uniform standard based on expert opinion (ACOG, AIUM, SMFM) EDD=280 days after first day LMP Half of women accurately remember LMP 40% adjustment in 1st trimester; 10% adjustment 2nd trimester Use earliest US