
SLIDE 1
30-31 Janvier 1er Février 2019
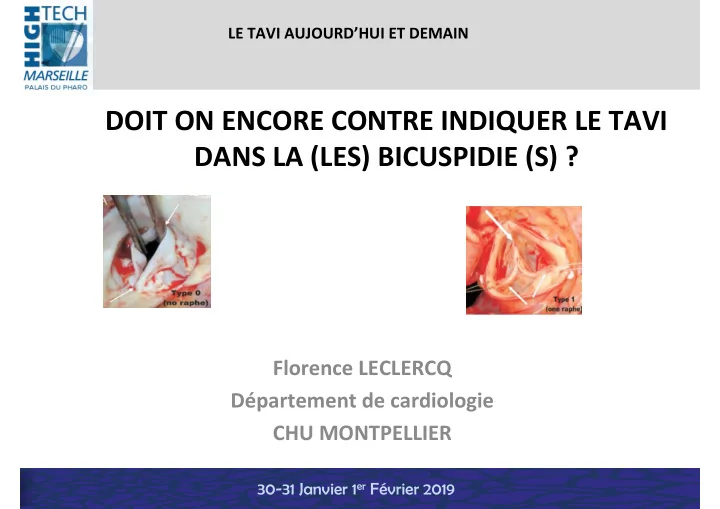
DOIT ON ENCORE CONTRE INDIQUER LE TAVI DANS LA (LES) BICUSPIDIE (S) ?
Florence LECLERCQ Département de cardiologie CHU MONTPELLIER
LE TAVI AUJOURD’HUI ET DEMAIN
DOIT ON ENCORE CONTRE INDIQUER LE TAVI DANS LA (LES) BICUSPIDIE (S) - - PowerPoint PPT Presentation
LE TAVI AUJOURDHUI ET DEMAIN DOIT ON ENCORE CONTRE INDIQUER LE TAVI DANS LA (LES) BICUSPIDIE (S) ? Florence LECLERCQ Dpartement de cardiologie CHU MONTPELLIER 30-31 Janvier 1 er Fvrier 2019 CONFLITS DINTERETS Subventions et
30-31 Janvier 1er Février 2019
LE TAVI AUJOURD’HUI ET DEMAIN
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019 Post-implantation aortic regurgitation (AR) ≥ grade 2 occurred in 28.4% but which appears to be mitigated (17.4%) by MSCT- based TAV sizing (performed in 2/3 patients)
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019
– Greater radial force : to circulate the native annulus and obliterating potential sites of paravalvular AR. – External skirt of the Sapien 3: decrease risk of paravalvular AR – calcified nodules or raphe: may impair complete prosthesis expansion – Potential risk of rupture ?
– Supra-annular position: potentially improve hemodynamic outcomes with non circular annulus – External wrap of the EVOLUT Pro: decrease risk of paravalvular AR – Reduced radial strength relative to balloon-expandable valve and frequent need to post dilatation
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019 2018
30-31 Janvier 1er Février 2019
30-31 Janvier 1er Février 2019
with high rates of device success and low rates of early safety events
required.
need to be defined.
new devices have to be evaluated
aortic anatomy