
SLIDE 1
Page 1
PTH analogs, alone and in combination with antiresorptives
Anne Schafer, MD
Associate Professor UCSF and the San Francisco VA Health Care System July 11, 2019
Research support from Bariatric Advantage and Tate & Lyle (supplements donated for research study)
Disclosures Treatment of osteoporosis
Antiresorptive agents Bisphosphonates Denosumab Raloxifene Calcitonin, estrogen Anabolic agents Teriparatide (PTH 1-34) Abaloparatide (PTHrP) Mixed anabolic and antiresorptive agent Romosozumab
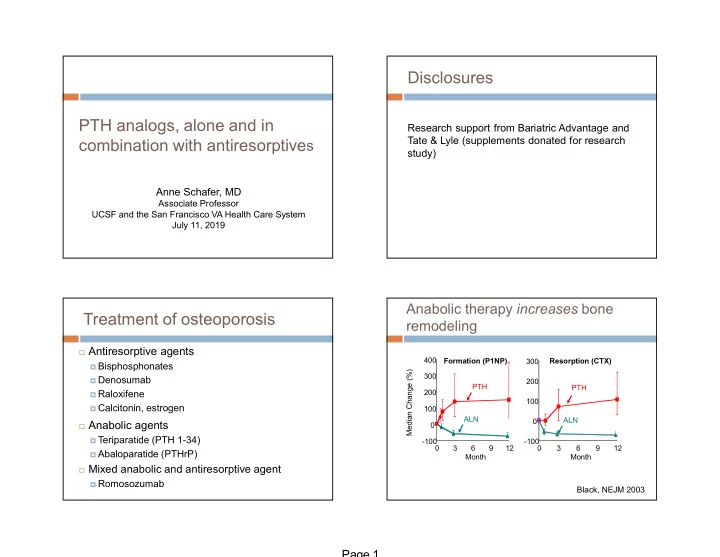
Anabolic therapy increases bone remodeling
Median Change (%)
- 100
100 200 300 3 6 9 12 Month
- 100
100 200 300 400 3 6 9 12 Month Resorption (CTX) Formation (P1NP) PTH ALN PTH ALN