
SLIDE 1
5/10/2013 1
- Dr. J.W. Scott’
’ ’ ’s parabola and the medical-industrial complex
Jesse B Jupiter MD Hansjorg Wyss/AO Professor Harvard Med
Disclosures
- Consultant Trimed Co
- AO Foundation
- Stock OHK Co
- Research AO foundation
- Reviewer Elsevier;Springer; Walter Klower
- Editor Walter Klower
- Committess AAHS;ASSH;AAOS
- All images in presentation are my own
I certify that, to the best of my knowledge, no aspect of my current personal
- r profession situation might reasonably be expected to affect significantly
my views on the subject on which I am presenting.
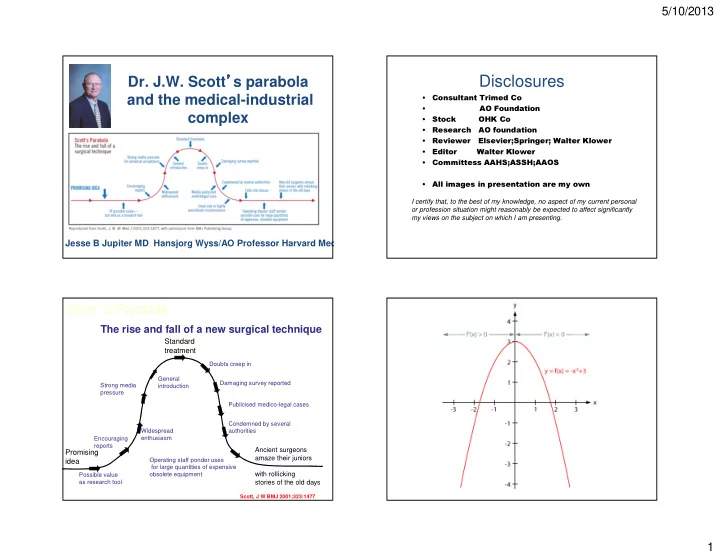
Scott’s Parabola
The rise and fall of a new surgical technique
Promising idea Standard treatment
Possible value as research tool Encouraging reports Widespread enthusiasm Strong media pressure General introduction Doubts creep in Damaging survey reported Publicised medico-legal cases Condemned by several authorities Operating staff ponder uses for large quantities of expensive
- bsolete equipment
Ancient surgeons amaze their juniors with rollicking stories of the old days
Scott, J W BMJ 2001;323:1477