
SLIDE 1
4/4/2014 1
Hybrid Repair for Aortic Pathology: A Reasonable Option in Selected Patients
William J. Quinones-Baldrich MD Professor of Surgery Director UCLA Aortic Center UCLA Medical Center Los Angeles, California
Disclosures
- Off label use will be presented
- Device companies not promote or assure
safety and efficacy of off label use of their products
- Speaker/consultant
W.L. Gore Endologix Medtronic
Hybrid Repair for Aortic Pathology
- Rationale: Reduce magnitude of surgical
intervention
- Thoraco-abdominal aorta
- Aortic Arch
- Use currently available endovascular devices
- Allow treatment of complex pathology in high
risk patients
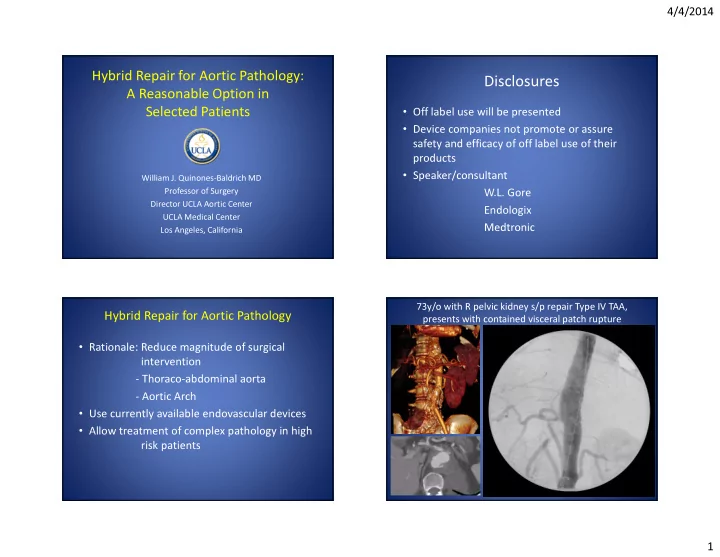
73y/o with R pelvic kidney s/p repair Type IV TAA, presents with contained visceral patch rupture