
SLIDE 1
2/16/2018 1
Difficult Diagnosis
- E. ALEXANDRA BROWN, MD
ASSISTANT PROFESSOR OF NEUROLOGY, UCSF DIRECTOR, ZUCKERBERG SAN FRANCISCO GENERAL NEUROLOGY CLINIC
Disclosures
I have nothing to disclose.
54F with 6 month history of headache
- Out of medical care x 7 years
- Headaches are 2-3 days per month
- Pulsating, severe, bitemporal location
- Nausea, photophobia, phonophobia
- Previously relieved by rest and OTCs
- OTCs no longer help
- Neuro exam reportedly normal per PCP
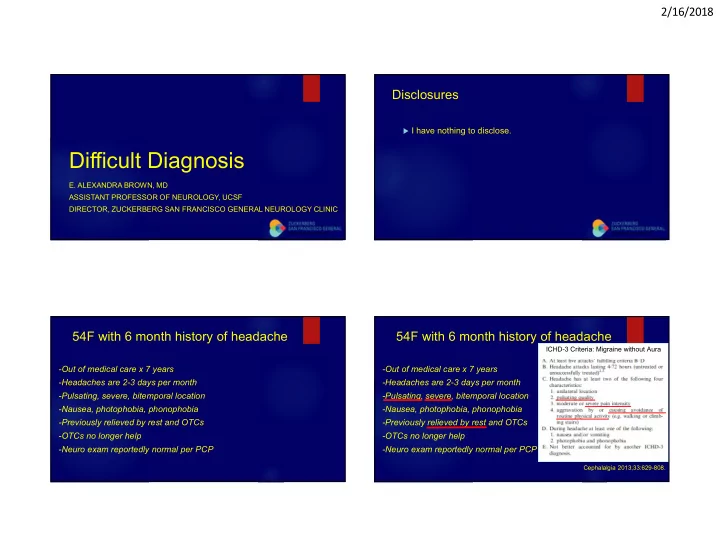
54F with 6 month history of headache
- Out of medical care x 7 years
- Headaches are 2-3 days per month
- Pulsating, severe, bitemporal location
- Nausea, photophobia, phonophobia
- Previously relieved by rest and OTCs
- OTCs no longer help
- Neuro exam reportedly normal per PCP
Cephalalgia 2013;33:629-808.
ICHD-3 Criteria: Migraine without Aura