
SLIDE 1
Page 1
NEUROCRITICAL CARE PROGRAM
UC SF
Cryptogenic Strokes: Evaluation and Management
- J. Claude Hemphill III, MD, MAS
Kenneth Rainin Chair in Neurocritical Care Professor of Neurology and Neurological Surgery University of California, San Francisco Chief of Neurology, San Francisco General Hospital Past-President, Neurocritical Care Society
Disclosures Research Support: NIH/NINDS; Cerebrotech Medical Stock (options): Ornim
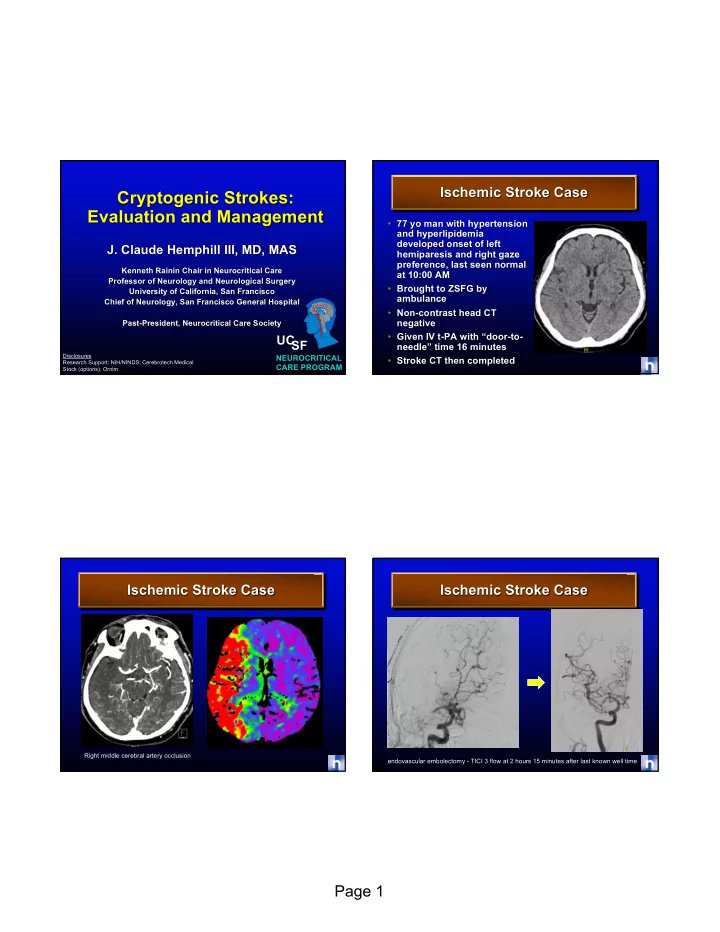
Ischemic Stroke Case
- 77 yo man with hypertension
and hyperlipidemia developed onset of left hemiparesis and right gaze preference, last seen normal at 10:00 AM
- Brought to ZSFG by
ambulance
- Non-contrast head CT
negative
- Given IV t-PA with “door-to-
needle” time 16 minutes
- Stroke CT then completed
Ischemic Stroke Case
Right middle cerebral artery occlusion
Ischemic Stroke Case
endovascular embolectomy - TICI 3 flow at 2 hours 15 minutes after last known well time