
SLIDE 1
Colorectal Cancer Screening: Colonoscopy, Potential and Pitfalls
Jonathan P. Terdiman, M.D. Professor of Clinical Medicine University of California, San Francisco
Disclosures: None CRC: still a major public health problem
- 1 million cases per year worldwide
and ½ million deaths
- USA
– 4th most common cancer ~ 150, 000 cases per year – 2nd most common cause of cancer death ~ 50, 000/yr – Lifetime risk is 3-6%
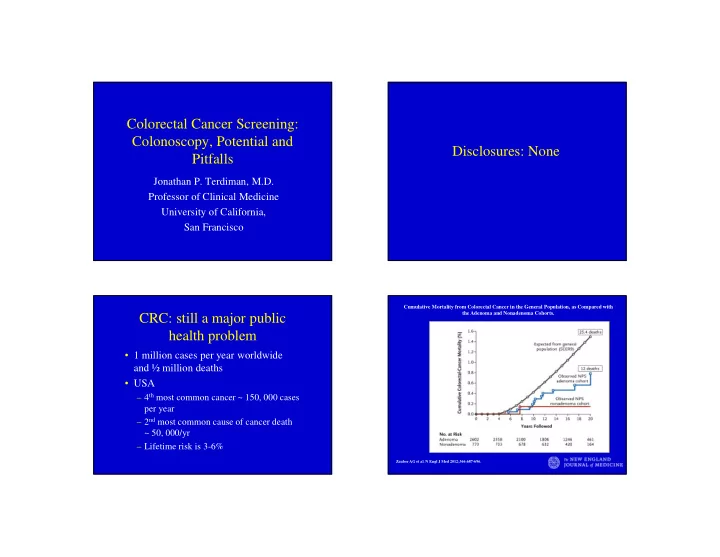
Cumulative Mortality from Colorectal Cancer in the General Population, as Compared with the Adenoma and Nonadenoma Cohorts.
Zauber AG et al. N Engl J Med 2012;366:687-696.