
SLIDE 1
5/22/19 1
An Evidence Based Approach to Colorectal Cancer Screening
Jay Ryan, M.D. Associate Professor of Medicine UCSF 5/22/2019
No Disclosures
Colorectal Cancer
- Lifetime incidence of 6%
- Prevalence of 1% in asymptomatic patients aged 50-75
- Common cause of cancer death, 2nd in men, 3rd in women
- Well defined precursor lesion (adenoma) with long lag time
until the development of cancer
- Reasonable target for screening
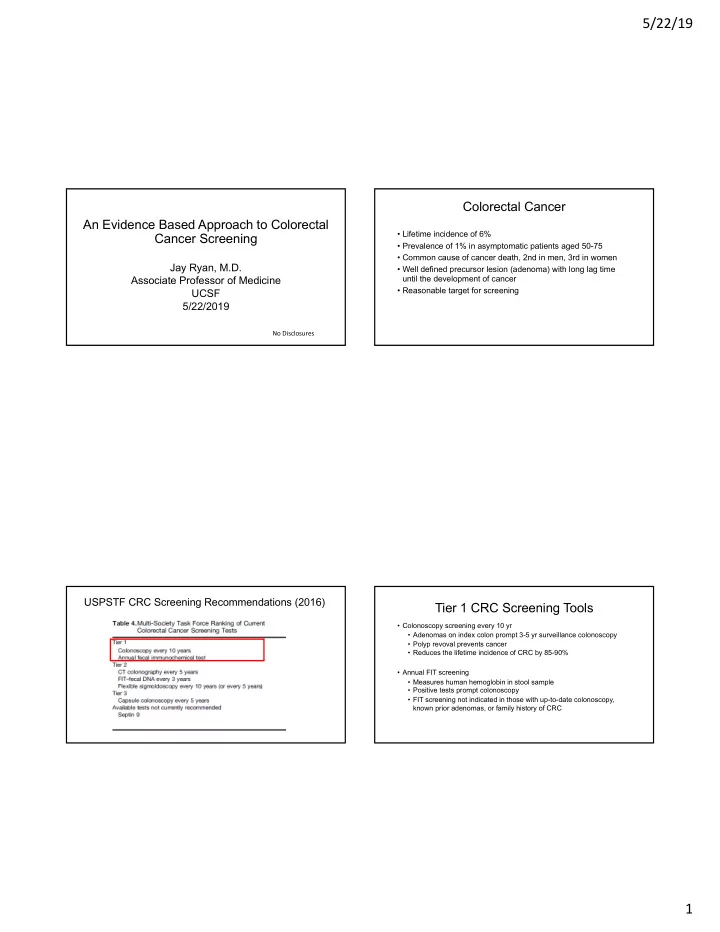
USPSTF CRC Screening Recommendations (2016)
Tier 1 CRC Screening Tools
- Colonoscopy screening every 10 yr
- Adenomas on index colon prompt 3-5 yr surveillance colonoscopy
- Polyp revoval prevents cancer
- Reduces the lifetime incidence of CRC by 85-90%
- Annual FIT screening
- Measures human hemoglobin in stool sample
- Positive tests prompt colonoscopy
- FIT screening not indicated in those with up-to-date colonoscopy,
known prior adenomas, or family history of CRC