
SLIDE 1
tdp-43
Ann C. McKee M.D.
Professor of Neurology and Pathology Boston University School of Medicine
Director, Neuropathology, New England Veterans Healthcare System and Brain Banks
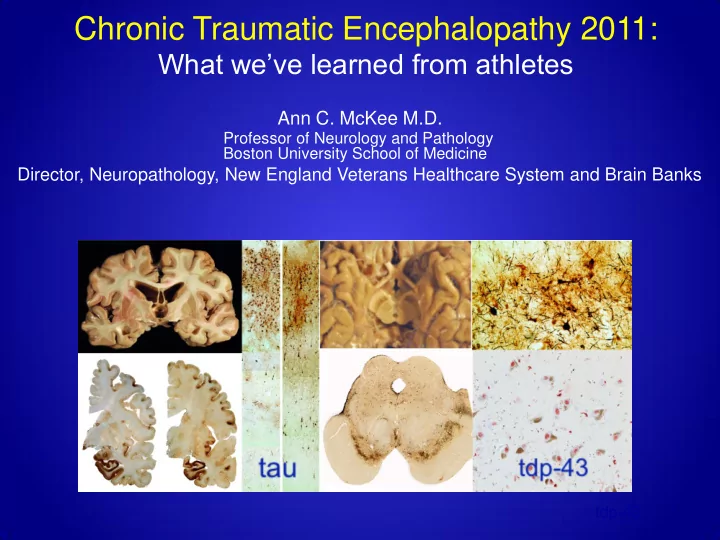
Chronic Traumatic Encephalopathy 2011: What weve learned from - - PowerPoint PPT Presentation
Chronic Traumatic Encephalopathy 2011: What weve learned from athletes Ann C. McKee M.D. Professor of Neurology and Pathology Boston University School of Medicine Director, Neuropathology, New England Veterans Healthcare System and Brain
tdp-43
Ann C. McKee M.D.
Professor of Neurology and Pathology Boston University School of Medicine
Director, Neuropathology, New England Veterans Healthcare System and Brain Banks
2
Over the past 3.5 years, the the brains and spinal cords
have been donated to the VA MTBI Brain Bank
temporary states of neuronal and axonal derangement
mTBI, including concussion and subconcussive blows, but evolves slowly
and cytoskeletal disturbances that trigger the pathological cascade that leads to CTE.
Harrison S. Martland (1883-1954) First full time paid pathologist Newark city Hospital 1909- 1927 Chief Medical examiner Essex county
First reported by Martland in 1928 in Boxers Punch drunk. JAMA 91:1103–1107, 1928 Martland described the spectrum of abnormalities found in "nearly one half of the fighters who have stayed in the game long enough” In 2009, in the worlds literature: 51 cases of CTE including 3 cases from BU
Chronic Traumatic Encephalopathy in Athletes: Progressive Tauopathy following Repetitive Head Injury.
McKee et al. J Neuropath Exp Neurol, 2009 68(7): 709-735
Control
Abnormal tau protein
Neurofibrillary tangles CTE Normal
Inclusions and neurites
6
>150 subjects; >70 cognitively intact Longitudinally assessed since 1948
68 year old man
Half-brain sections Immunostained for hyperphosphorylated tau protein
CTE
Hyperphosphorylated tau protein
perivascular
depths of the sulcus Hyperphosphorylated tau protein as Neuronal and Glial tangles Unlike any other tauopathy
CTE
superficial layers glial tangles
Normal CTE Alzheimer’s disease No Tau, no Aß Tau, no Aß Tau and Aß
11
Houston Oilers 1984-1990 Miami Dolphins 1991-1993
attention, concentration, judgment, and ability to multitask.
gunshot wound
13
Began playing football at age 8 24 total seasons, safety in college and pro > 10 concussions 11-year NFL career Several concussions with loss of consciousness Never admitted to hospital No known brain trauma since retiring from Post-NFL, very successful in food supply industry ( Duerson Foods) Very active in NFLPA; Benefits Board General health: very good Work and financial difficulties began in 2007 No history of depression or other psychiatric difficulties; no substance abuse
14
difficulties, as well as problems with language and “vision”
Short fuse Hot tempered Physically abusive Verbally abusive
Suicide at age 21. Recent stress and academic decline.
17
>10 concussions, multiple cervical spine injuries
fasciculations, spasticity Dx: ALS
TDP+ inclusions in motor neurons of brain and cord (CTEM)
may develop a motor neuron disease
1960 and 2010 was associated with a RR of 2.25 for being clinically diagnosed with ALS compared to age and gender matched controls.
Alzheimer’s disease, that we are finding in the brains of many professional football players, boxers, veterans and hockey players.
repeated mTBI that most commonly occurs in an individual’s teens and early twenties.
decades to involve widespread degeneration of many brain structures.
prominent early personality and behavioral changes (short fuse, depression, suicidal ideations, impulsivity) and memory loss. There is a slow deterioration that progresses to include dementia, parkinsonism, gait and speech disorders.
develop a motor neuron disease, CTEM
cortex, especially motor cortex, the subcortical white matter, basal ganglia, diencephalon, brainstem and spinal cord.
individuals with CTE, as a result, their cognitive and behavioral symptoms also tend to be less severe
management of mTBI in sports and military will decrease the frequency
systems and beginning preclinical therapeutic trials
24
Victor Alvarez Christine Baugh Andrew Budson Kerry Cormier Dan Daneshvar Brandon Gavett. Lee Goldstein Garth Hall
all individuals from: Boston University CSTE Boston University Framingham Heart Study Boston University Alzheimer’s Disease Center
And all the veterans, athletes and families who participated in our research
Neil Kowall Carol Kubilus Lisa McHale David Riley Hyo Soon-Lee Prince Williams Ben Wolozin Sydney Wojtowicz
25