
SLIDE 1
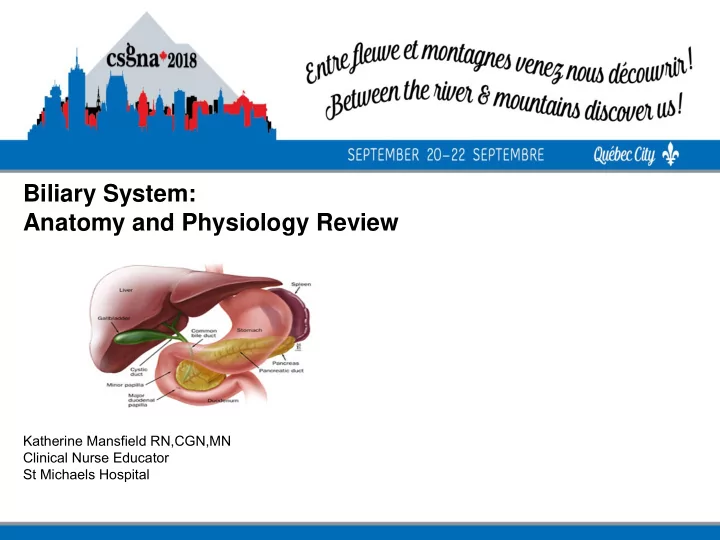
Biliary System: Anatomy and Physiology Review
Katherine Mansfield RN,CGN,MN Clinical Nurse Educator St Michaels Hospital
Biliary System: Anatomy and Physiology Review Katherine Mansfield - - PowerPoint PPT Presentation
Biliary System: Anatomy and Physiology Review Katherine Mansfield RN,CGN,MN Clinical Nurse Educator St Michaels Hospital Objectives To review the anatomy and physiology of the Biliary System To consider the main functions of the
Katherine Mansfield RN,CGN,MN Clinical Nurse Educator St Michaels Hospital
Black Pigment stones contain bilirubin polymers & inorganic calcium salts
Cholecystitis or pancreatitis)
– New drug therapy to dissolve stones Ursodiol, (Actigall)
– Infusion of methyl tertbutyl ether into gallbladder to
– Biliary lithotripsy (acoustic shock waves) – No medical treatment for pigment stones – Surgery only option for pigment stones
Nasobiliary Catheter
EUS
– Agenesis = absence of gallbladder – Anomalies of location – Ectopic gallbladder – need
– Anomalies of form more than 1 cystic structure
– Anomalies of f i
– Anomalies of extrahepatic duct conf i
– Cystic anomalies of CBD choledochal cyst
– Cystic dilatation of intrahepatic ducts or “Caroli’s