
SLIDE 1
4/18/2015 1
Aortoiliac occlusive disease
Bala Ramanan, MBBS 1st year vascular surgery fellow
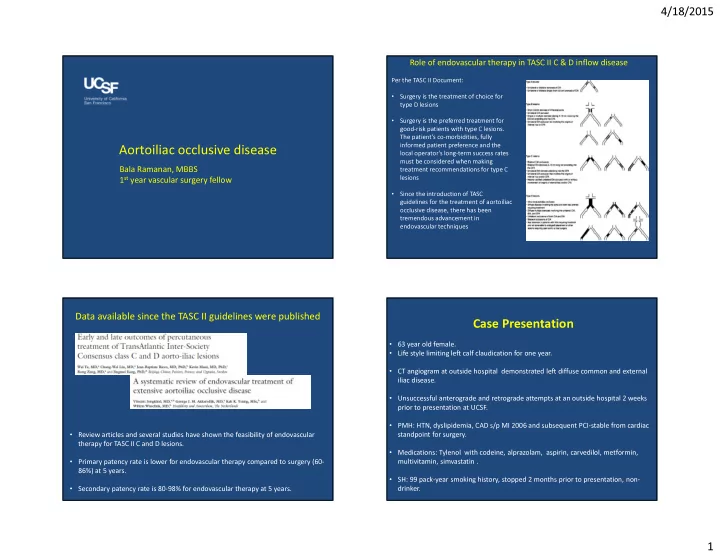
Per the TASC II Document:
- Surgery is the treatment of choice for
type D lesions
- Surgery is the preferred treatment for
good-risk patients with type C lesions. The patient's co-morbidities, fully informed patient preference and the local operator's long-term success rates must be considered when making treatment recommendations for type C lesions
- Since the introduction of TASC
guidelines for the treatment of aortoiliac
- cclusive disease, there has been
tremendous advancement in endovascular techniques
Role of endovascular therapy in TASC II C & D inflow disease
Data available since the TASC II guidelines were published
- Review articles and several studies have shown the feasibility of endovascular
therapy for TASC II C and D lesions.
- Primary patency rate is lower for endovascular therapy compared to surgery (60-
86%) at 5 years.
- Secondary patency rate is 80-98% for endovascular therapy at 5 years.
Case Presentation
- 63 year old female.
- Life style limiting left calf claudication for one year.
- CT angiogram at outside hospital demonstrated left diffuse common and external
iliac disease.
- Unsuccessful anterograde and retrograde attempts at an outside hospital 2 weeks
prior to presentation at UCSF.
- PMH: HTN, dyslipidemia, CAD s/p MI 2006 and subsequent PCI-stable from cardiac
standpoint for surgery.
- Medications: Tylenol with codeine, alprazolam, aspirin, carvedilol, metformin,
multivitamin, simvastatin .
- SH: 99 pack-year smoking history, stopped 2 months prior to presentation, non-