
SLIDE 1
Whole Person Care in a Behavioral Health Setting
Phase 1 Webinar Series CPAA/AIMS Center Training Program January 15, 2019
AIMS Center Introductions
Sara Barker, MPH
Assistant Director for Implementation
John Kern, MD
Clinical Professor
Juliann Salisbury
Program Coordinator
Introductions
- Organization, Team Member Names & Roles
- What do you hope to get out of our training
year together?
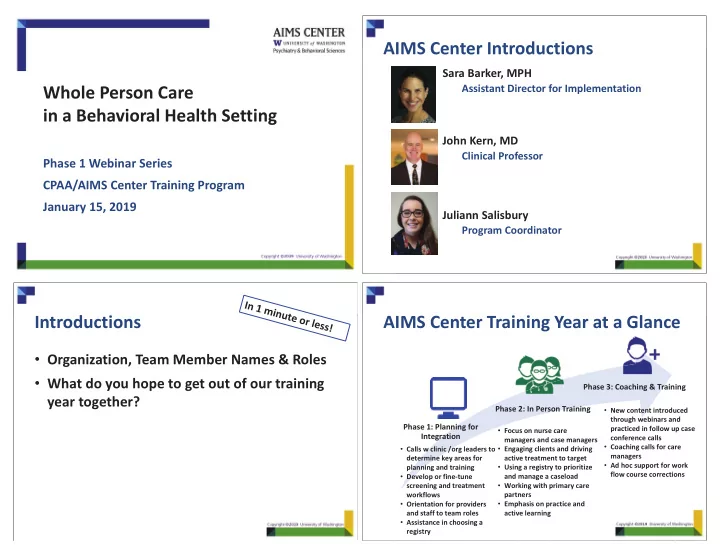
AIMS Center Training Year at a Glance
Phase 1: Planning for Integration Phase 2: In Person Training Phase 3: Coaching & Training
- Calls w clinic /org leaders to
determine key areas for planning and training
- Develop or fine-tune
screening and treatment workflows
- Orientation for providers
and staff to team roles
- Assistance in choosing a
registry
- Focus on nurse care
managers and case managers
- Engaging clients and driving
active treatment to target
- Using a registry to prioritize
and manage a caseload
- Working with primary care
partners
- Emphasis on practice and
active learning
- New content introduced
through webinars and practiced in follow up case conference calls
- Coaching calls for care
managers
- Ad hoc support for work
flow course corrections