
SLIDE 1
Abstract Session C2: Women's Health Moderators: Wendy L. Bennett, MD, MPH Discussant: Melissa McNeil, MD, MPH, SGIM 2014 Distinguished Professor in Women’s Health
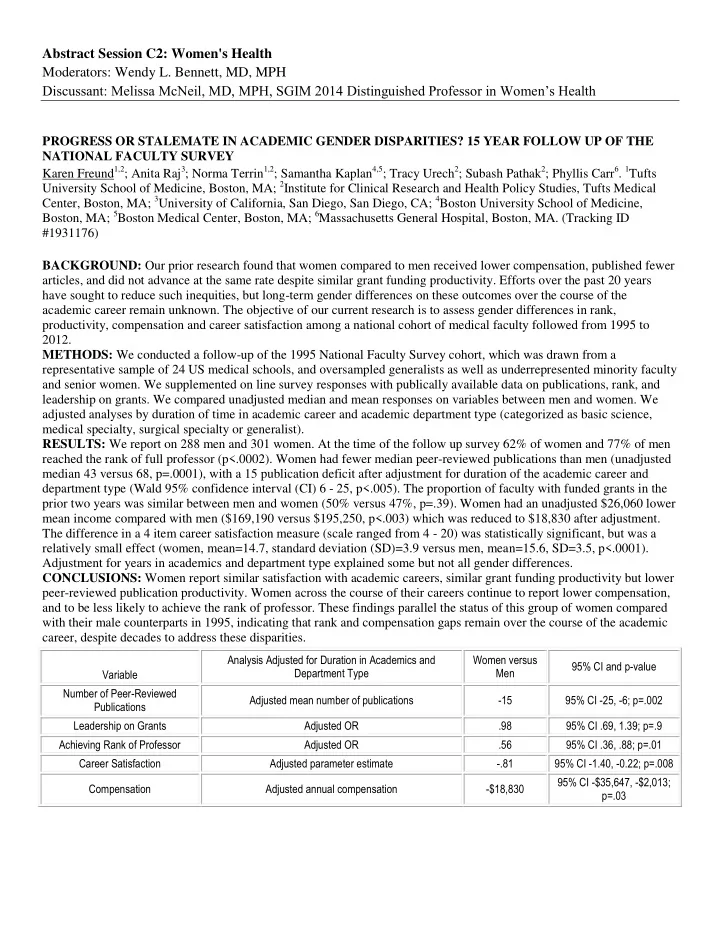
PROGRESS OR STALEMATE IN ACADEMIC GENDER DISPARITIES? 15 YEAR FOLLOW UP OF THE NATIONAL FACULTY SURVEY Karen Freund1,2; Anita Raj3; Norma Terrin1,2; Samantha Kaplan4,5; Tracy Urech2; Subash Pathak2; Phyllis Carr6. 1Tufts University School of Medicine, Boston, MA; 2Institute for Clinical Research and Health Policy Studies, Tufts Medical Center, Boston, MA; 3University of California, San Diego, San Diego, CA; 4Boston University School of Medicine, Boston, MA; 5Boston Medical Center, Boston, MA; 6Massachusetts General Hospital, Boston, MA. (Tracking ID #1931176) BACKGROUND: Our prior research found that women compared to men received lower compensation, published fewer articles, and did not advance at the same rate despite similar grant funding productivity. Efforts over the past 20 years have sought to reduce such inequities, but long-term gender differences on these outcomes over the course of the academic career remain unknown. The objective of our current research is to assess gender differences in rank, productivity, compensation and career satisfaction among a national cohort of medical faculty followed from 1995 to 2012. METHODS: We conducted a follow-up of the 1995 National Faculty Survey cohort, which was drawn from a representative sample of 24 US medical schools, and oversampled generalists as well as underrepresented minority faculty and senior women. We supplemented on line survey responses with publically available data on publications, rank, and leadership on grants. We compared unadjusted median and mean responses on variables between men and women. We adjusted analyses by duration of time in academic career and academic department type (categorized as basic science, medical specialty, surgical specialty or generalist). RESULTS: We report on 288 men and 301 women. At the time of the follow up survey 62% of women and 77% of men reached the rank of full professor (p<.0002). Women had fewer median peer-reviewed publications than men (unadjusted median 43 versus 68, p=.0001), with a 15 publication deficit after adjustment for duration of the academic career and department type (Wald 95% confidence interval (CI) 6 - 25, p<.005). The proportion of faculty with funded grants in the prior two years was similar between men and women (50% versus 47%, p=.39). Women had an unadjusted $26,060 lower mean income compared with men ($169,190 versus $195,250, p<.003) which was reduced to $18,830 after adjustment. The difference in a 4 item career satisfaction measure (scale ranged from 4 - 20) was statistically significant, but was a relatively small effect (women, mean=14.7, standard deviation (SD)=3.9 versus men, mean=15.6, SD=3.5, p<.0001). Adjustment for years in academics and department type explained some but not all gender differences. CONCLUSIONS: Women report similar satisfaction with academic careers, similar grant funding productivity but lower peer-reviewed publication productivity. Women across the course of their careers continue to report lower compensation, and to be less likely to achieve the rank of professor. These findings parallel the status of this group of women compared with their male counterparts in 1995, indicating that rank and compensation gaps remain over the course of the academic career, despite decades to address these disparities.
Variable Analysis Adjusted for Duration in Academics and Department Type Women versus Men 95% CI and p-value Number of Peer-Reviewed Publications Adjusted mean number of publications
- 15
95% CI -25, -6; p=.002 Leadership on Grants Adjusted OR .98 95% CI .69, 1.39; p=.9 Achieving Rank of Professor Adjusted OR .56 95% CI .36, .88; p=.01 Career Satisfaction Adjusted parameter estimate
- .81
95% CI -1.40, -0.22; p=.008 Compensation Adjusted annual compensation
- $18,830