
SLIDE 1
9/12/2019 1
- 1. Beta blockers (Sotalol)
- 2. Amiodarone
- 3. Catheter ablation
- 4. AICD
M S
ARVD Therapy
Treatment for patients with ARVC
- Early drug trials involved small groups with different follow up periods
- Cohorts were inhomogeneous and involved those with sustained and
unsustained VT
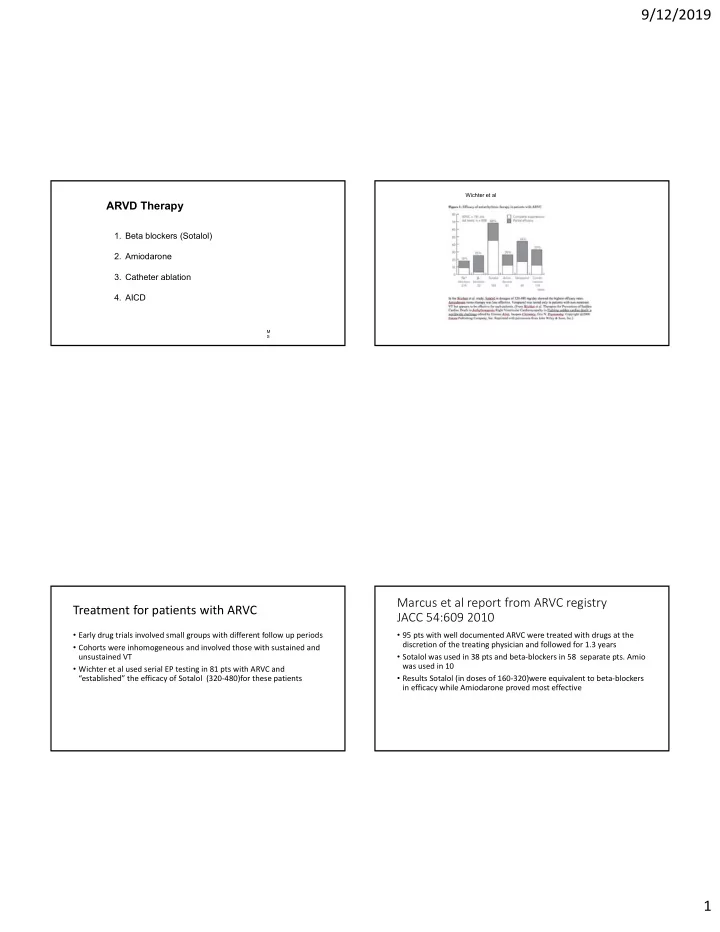
- Wichter et al used serial EP testing in 81 pts with ARVC and
“established” the efficacy of Sotalol (320‐480)for these patients
Wichter et al
Marcus et al report from ARVC registry JACC 54:609 2010
- 95 pts with well documented ARVC were treated with drugs at the
discretion of the treating physician and followed for 1.3 years
- Sotalol was used in 38 pts and beta‐blockers in 58 separate pts. Amio
was used in 10
- Results Sotalol (in doses of 160‐320)were equivalent to beta‐blockers