
Incorporating DecisionDx-Melanoma into Clinical Practice:
Molecular Information for Personalized Management Decisions
Eric D. Whitman, MD, FACS Medical Director, Atlantic Health System Cancer Care Director, Atlantic Melanoma Center Morristown and Summit, New Jersey
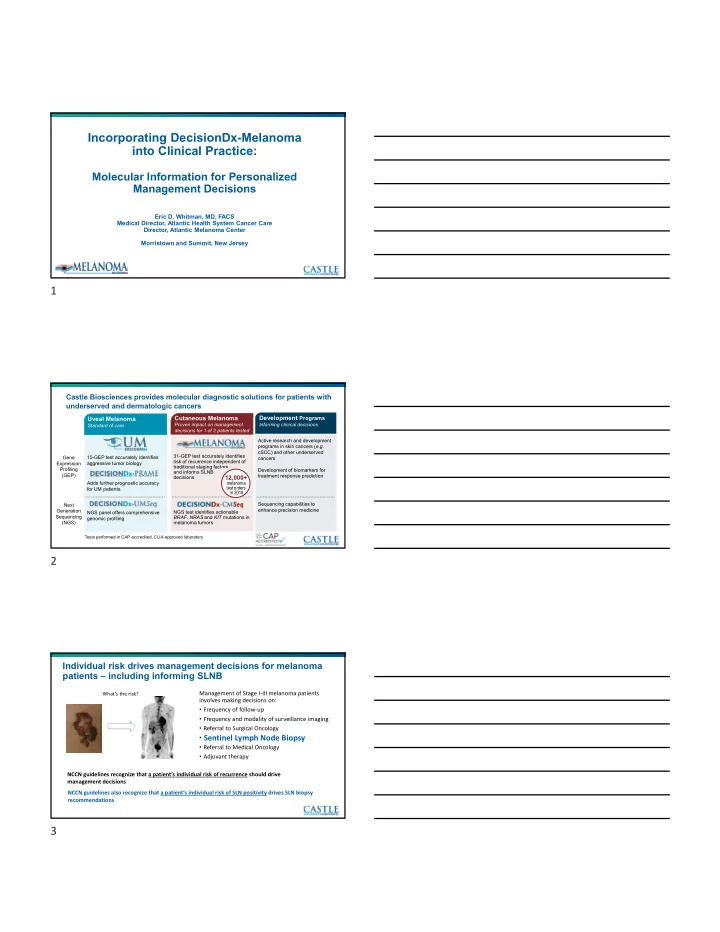
Castle Biosciences provides molecular diagnostic solutions for patients with underserved and dermatologic cancers
15-GEP test accurately identifies aggressive tumor biology Adds further prognostic accuracy for UM patients NGS panel offers comprehensive genomic profiling
Uveal Melanoma
Standard of care 31-GEP test accurately identifies risk of recurrence independent of traditional staging factors and informs SLNB decisions NGS test identifies actionable BRAF, NRAS and KIT mutations in melanoma tumors
Cutaneous Melanoma
Proven impact on management decisions for 1 of 2 patients tested Active research and development programs in skin cancers (e.g. cSCC) and other underserved cancers Development of biomarkers for treatment response prediction Sequencing capabilities to enhance precision medicine
Development Programs
Informing clinical decisions Gene Expression Profiling (GEP) Next Generation Sequencing (NGS)
12,000+
melanoma test orders in 2018
Tests performed in CAP-accredited, CLIA-approved laboratory
Individual risk drives management decisions for melanoma patients – including informing SLNB
Management of Stage I‐III melanoma patients involves making decisions on:
- Frequency of follow‐up
- Frequency and modality of surveillance imaging
- Referral to Surgical Oncology
- Sentinel Lymph Node Biopsy
- Referral to Medical Oncology
- Adjuvant therapy
What’s the risk?
NCCN guidelines recognize that a patient’s individual risk of recurrence should drive management decisions
Sentinel Lymph Node Biopsy
NCCN guidelines also recognize that a patient’s individual risk of SLN positivity drives SLN biopsy recommendations