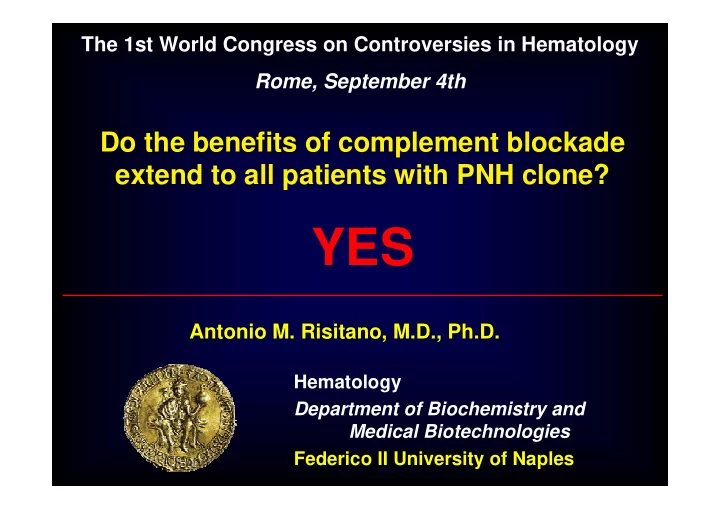
SLIDE 8 Patient Age Years from diagnosis Treatment duration (months) LDH before Ecu LDH during Ecu Hb before Ecu Hb during Ecu Hb gain PNH RBC before Ecu (%) PNH RBC during Ecu (%) 1 41 15 17 680 225 10 12,8 +2,8 n.a. 48 2 25 2 18 1216 356 7,5 10 +2,5 23 60 3 51 10 16 727 250 9,3 10,5 +1,2 40 89 4 16 1 1 1425 342 7,3 9 +1,7 10 24 5 50 7 39 3968 860 8 10 +2 19 89 6 59 17 4 3100 290 7 11,6 +4,6 50 n.a. 7 39 10 5 2190 250 10,7 11,5 +0,8 46 48 8 38 3 18 1500 360 9 10,7 +1,7 12 45 9 16 1 9 2100 250 9 11,7 +2,7 13 52 Mean 37 6,1 14,1 1878 353 8 10 +2,2 26,6 58,1 Median 39 5 16 1500 290 9 10,7 +2 21 52
ECULIZUMAB IN NON TRANSFUSED PATIENTS
An Italian pilot experience (Risitano et al, EHA 2009) Terminal complement inhibition by eculizumab in non transfused PNH patients leads to improvement of most clinical manifestations, including symptoms of intravascular hemolysis and anemia