SLIDE 14 15-‑03-‑31 ¡ 14 ¡
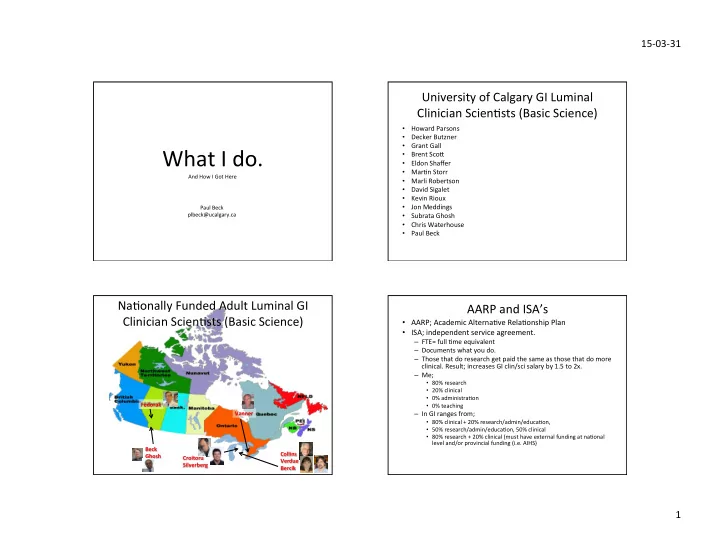
RI ¡ RII ¡ TGFβ ¡
kinase ¡
2 ¡ 3 ¡ Smad ¡ 4 ¡ Smad ¡ nucleus ¡ DN ¡
Smad ¡ 7 ¡
2 ¡ p ¡ 3 ¡ Beck ¡et ¡al ¡Am ¡J ¡Path ¡2003 ¡ ¡
Blockade ¡in ¡ ¡TGFβ ¡Signaling ¡Exacerbates ¡ ColiJs ¡and ¡Delays ¡Recovery ¡
TGFβ ¡DN ¡ Wt ¡ ¡ Day ¡7 ¡DSS ¡ Day ¡10 ¡post-‑DSS ¡
These ¡and ¡other ¡studies ¡led ¡to ¡the ¡ development ¡of ¡an@-‑SMAD7 ¡therapy ¡ now ¡in ¡clinical ¡trials ¡in ¡IBD! ¡
Papers ¡from ¡Post-‑doc ¡12+4 ¡
1. Beck ¡PL, ¡Xavier ¡R, ¡Podolsky ¡DK, ¡Seed ¡B. ¡Mechanisms ¡of ¡NSAID-‑induced ¡gastrointesJnal ¡injury ¡defined ¡using ¡mutant ¡mice. ¡ Gastroenterology ¡2000;119:699-‑705. ¡ 2. Beck ¡PL, ¡Taupin ¡D, ¡Kinoshita, ¡Podolsky ¡DK. ¡IntesJnal ¡trefoil ¡factors ¡alters ¡the ¡course ¡of ¡chemotherapy ¡and ¡radiotherapy-‑induced ¡ intesJnal ¡damage. ¡Proceeding ¡of ¡the ¡InternaJonal ¡MeeJng ¡On ¡RadiaJon ¡Induced ¡Injury, ¡RoOerdam ¡1998. ¡ 3. Beck ¡PL, ¡Podolsky ¡DK. ¡Growth ¡factors ¡in ¡inflammatory ¡bowel ¡disease. ¡ ¡Inflammatory ¡Bowel ¡Diseases ¡1999; ¡5(1): ¡44-‑60. ¡ ¡ 4. Itoh ¡H*, ¡Beck ¡PL*, ¡Inoe ¡N, ¡Podolsky ¡DK. ¡A ¡paradoxical ¡reducJon ¡in ¡suscepJbility ¡to ¡colonic ¡injury ¡upon ¡targeted ¡transgenic ¡ ablaJon ¡of ¡goblet ¡cells. ¡J. ¡Clin. ¡Invest. ¡1999 ¡104:1539-‑1547 ¡(* ¡co-‑first ¡authors). ¡ ¡ 5. Andres ¡PG, ¡Beck ¡PL, ¡Mizoguchi ¡E, ¡Mizoguchi ¡A, ¡Bhan ¡AK, ¡Dawson ¡T, ¡Kuziel ¡WA, ¡Maeda ¡N, ¡MacDermoO ¡RP, ¡Podolsky ¡DK, ¡Reinecker ¡
- HC. ¡ ¡Mice ¡with ¡a ¡SelecJve ¡DeleJon ¡of ¡the ¡CC ¡Chemokine ¡Receptors ¡5 ¡or ¡2 ¡are ¡Protected ¡from ¡Dextran ¡Sodium ¡Sulfate-‑Mediated ¡
ColiJs: ¡ ¡Lack ¡of ¡CC ¡Chemokine ¡Receptor ¡5 ¡Expression ¡Results ¡in ¡a ¡NK1.1+ ¡Lymphocyte-‑Associated ¡Immune ¡Response ¡in ¡the ¡
- IntesJne. ¡J ¡Immunol ¡2000; ¡174(12): ¡6303-‑6312. ¡
6. ¡Fox ¡JG, ¡Beck ¡P, ¡Dangler ¡CA, ¡Whary ¡MT, ¡Wang ¡TC, ¡Shi ¡HN, ¡Nagler-‑Anderson ¡C. ¡Concurrent ¡enteric ¡helminth ¡infecJon ¡modulates ¡ inflammaJon ¡and ¡gastric ¡immune ¡responses ¡and ¡reduces ¡Helicobacter-‑induced ¡gastric ¡atrophy. ¡Nat ¡Med ¡2000; ¡6(5):536-‑542. ¡ 7. ¡Cario ¡E, ¡Rosenberg ¡I, ¡Brandwein ¡S, ¡Beck ¡PL, ¡Reinecker ¡HC, ¡Podolsky ¡DK. ¡ ¡Lipopolysaccharide ¡acJvates ¡disJnct ¡signaling ¡pathways ¡ in ¡intesJnal ¡epithelial ¡cell ¡lines ¡expressing ¡toll-‑like ¡receptors. ¡J ¡Immunol ¡2000, ¡164: ¡966-‑972. ¡ 8. ¡Saubermann ¡LJ*, ¡Beck ¡P*, ¡De ¡Jong ¡YP, ¡Pitman ¡RS, ¡Ryan ¡MS, ¡Kim ¡HS, ¡Exley ¡M, ¡Snapper ¡S, ¡Balk ¡SP, ¡Hagen ¡SJ, ¡Kanauchi ¡O, ¡Motoki ¡K, ¡ Sakai ¡T, ¡Terhorst ¡C, ¡Koezuka ¡Y, ¡Pokolsky ¡DK, ¡Blumberg ¡RS. ¡AcJvaJon ¡of ¡Natural ¡Killer ¡T ¡Cells ¡by ¡Alpha-‑Galactosylceramide ¡in ¡the ¡ Presence ¡of ¡CD1d ¡Provides ¡ProtecJon ¡Against ¡ColiJs ¡in ¡Mice. ¡Gastroenterology ¡2000 ¡July; ¡119(1): ¡119-‑128 ¡*co-‑first ¡authors. ¡ 9. ¡Beck ¡PL, ¡Rosenberg ¡IM, ¡Xavier ¡RJ, ¡Koh ¡T, ¡Wong ¡JF, ¡Podolsky ¡DK ¡Transforming ¡Growth ¡Factor-‑beta ¡Mediates ¡IntesJnal ¡Healing ¡and ¡ SuscepJbility ¡to ¡Injury ¡in ¡Vitro ¡and ¡in ¡Vivo ¡Through ¡Epithelial ¡Cells. ¡Am ¡J ¡Pathol ¡2003 ¡Feb;162(2):597-‑608 ¡ 10. ¡Beck ¡PL, ¡Xavier ¡R, ¡Wong ¡J, ¡Ezedi ¡I, ¡Mashimo ¡H, ¡Mizoguchi ¡A, ¡Mizoguchi ¡E, ¡Bhan ¡AK, ¡Podolsky ¡DK. ¡ ¡Paradoxical ¡Roles ¡of ¡Different ¡ Nitric ¡Oxide ¡Synthase ¡Isoforms ¡in ¡Colonic ¡Injury. ¡ ¡Am ¡J ¡Physiol ¡Gastrointest ¡Liver ¡Physiol. ¡2004 ¡Jan; ¡286(1):G137-‑47. ¡ ¡ 11. ¡Beck ¡PL, ¡Wong ¡JF. ¡Li ¡Y, ¡Swaminathan ¡S, ¡Xavier ¡RJ, ¡Devaney ¡KL, ¡Podolsky ¡DK. ¡Chemotherapy ¡and ¡Radiotherapy-‑Induced ¡IntesJnal ¡ Damage ¡is ¡Regulated ¡by ¡IntesJnal ¡Trefoil ¡Factor. ¡Gastroenterology. ¡2004 ¡Mar; ¡126(3):796-‑808. ¡ 12. ¡Beck ¡PL, ¡Ihara ¡E, ¡Hirota ¡SA, ¡Macdonald ¡JA, ¡Meng ¡D, ¡Nanthakumar ¡NN, ¡Podolsky ¡DK, ¡Xavier ¡RJ. ¡Exploring ¡the ¡interplay ¡of ¡barrier ¡ funcJon ¡and ¡leukocyte ¡recruitment ¡in ¡intesJnal ¡inflammaJon ¡by ¡targeJng ¡fucosyltransferase ¡VII ¡and ¡trefoil ¡factor ¡3. ¡Am ¡J ¡Physiol ¡ Gastrointest ¡Liver ¡Physiol. ¡2010 ¡Jul;299(1):G43-‑53. ¡
Paul ¡Applying ¡for ¡a ¡Job! ¡
- PhD; ¡6 ¡papers, ¡1 ¡book ¡chapter ¡
- Med ¡School/Part ¡Jme ¡Post-‑doc; ¡14 ¡papers ¡
- Applying ¡for ¡CIHR/MRC; ¡17 ¡papers ¡ ¡
- Post-‑Doc; ¡12 ¡main, ¡4 ¡others ¡
- Applying ¡for ¡Job ¡1999 ¡(age ¡38); ¡
– ¡36 ¡published ¡or ¡in ¡press ¡ – AHFMR ¡grant ¡funded ¡ – Start ¡up ¡package….. ¡zero ¡
StarJng ¡on ¡Staff ¡1999 ¡ Find ¡Your ¡Confidence… ¡
perfect! ¡ ¡
everything ¡to ¡ everybody! ¡
– 100 ¡papers, ¡ 2000 ¡citaJons ¡ – Be ¡an ¡excellent ¡
¡