
SLIDE 1
5/26/2018 1
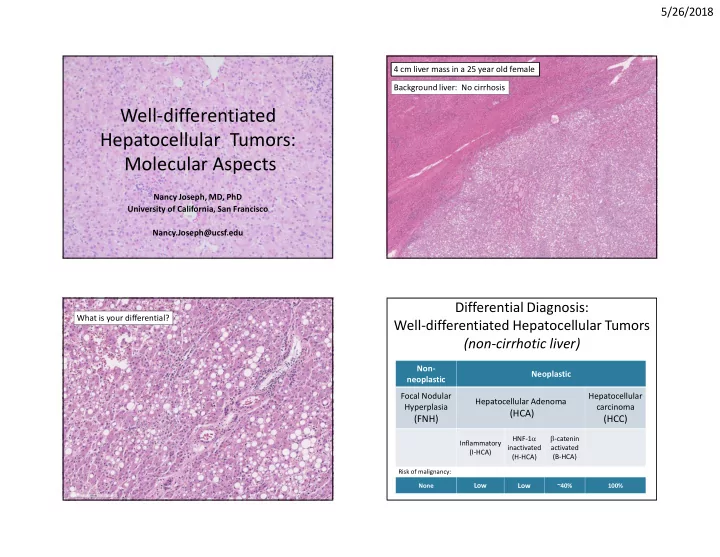
Well-differentiated Hepatocellular Tumors: Molecular Aspects
Nancy Joseph, MD, PhD University of California, San Francisco Nancy.Joseph@ucsf.edu 4 cm liver mass in a 25 year old female Background liver: No cirrhosis What is your differential? Non- neoplastic Neoplastic Focal Nodular Hyperplasia
(FNH)
Hepatocellular Adenoma
(HCA)
Hepatocellular carcinoma
(HCC)
Inflammatory (I-HCA) HNF-1a inactivated (H-HCA) b-catenin activated (B-HCA)
Differential Diagnosis: Well-differentiated Hepatocellular Tumors (non-cirrhotic liver)
Risk of malignancy: None
Low Low
~40% 100%