
SLIDE 1
5/7/2018 1
Intrahepatic cholangiocarcinoma
Histologic spectrum, novel markers and molecular assays
Sanjay Kakar, MD University of California, San Francisco
2018 Current Issues in Surgical Pathology Summary (not actual lecture)
Intrahepatic cholangiocarcinoma
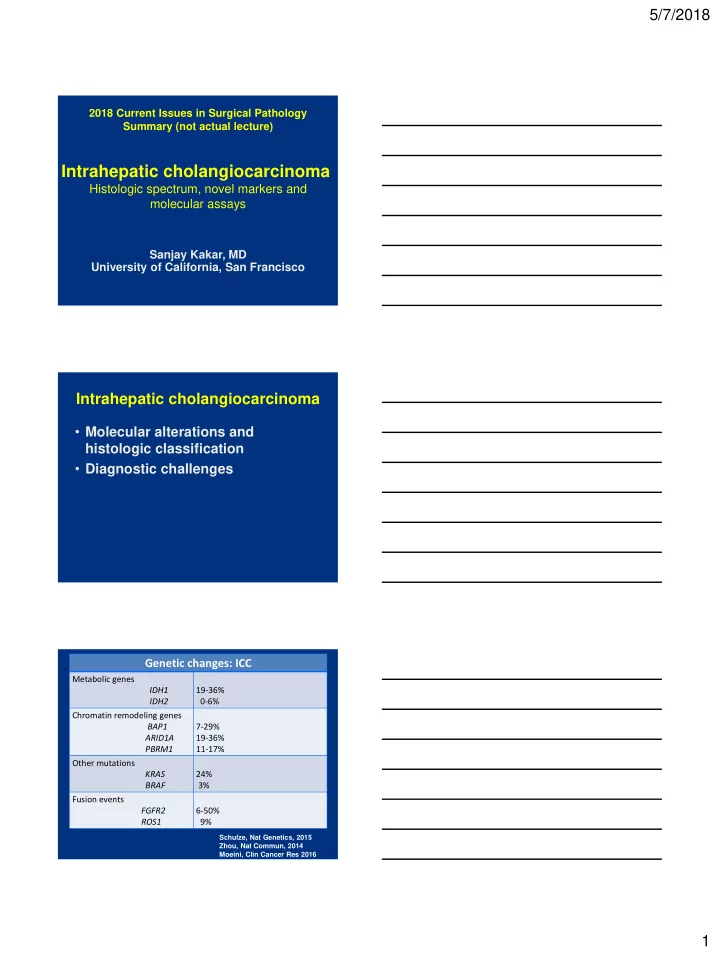
- Molecular alterations and
histologic classification
- Diagnostic challenges
Schulze, Nat Genetics, 2015 Zhou, Nat Commun, 2014 Moeini, Clin Cancer Res 2016