
7/22/2019 1
NELIA ADACI RN, BSN, CDONA, DNS-CT, RAC-CTA VP, The CHARTS Group
UNDERSTANDING PDPM
PDPM POLICIES; COMPONENTS; & MDS 3.0 CODING IN PDPM
GREATER NY HEALTHCARE FACILITIES ASSOCIATION
SNF QRP Provider Training | July/August2018 49
PROBLEMS WITH CURRENT MODEL: Payment is determined by volume of services provided rather than clinical characteristics of patient Index maximization causes patients with different comorbidities and costs, to still fall into the same RUG Non-Therapy Ancillaries (NTA) supplies and devices can be very costly, but are currently lumped in the Nursing payment TOO MANY ASSESSMENTS! CMS’ Goals: Create a model where payment is linked to clinical characteristics rather than volume of services or index maximization Create a separate NTA payment Reduce provider Burden
SNF QRP Provider Training | July/August2018 49
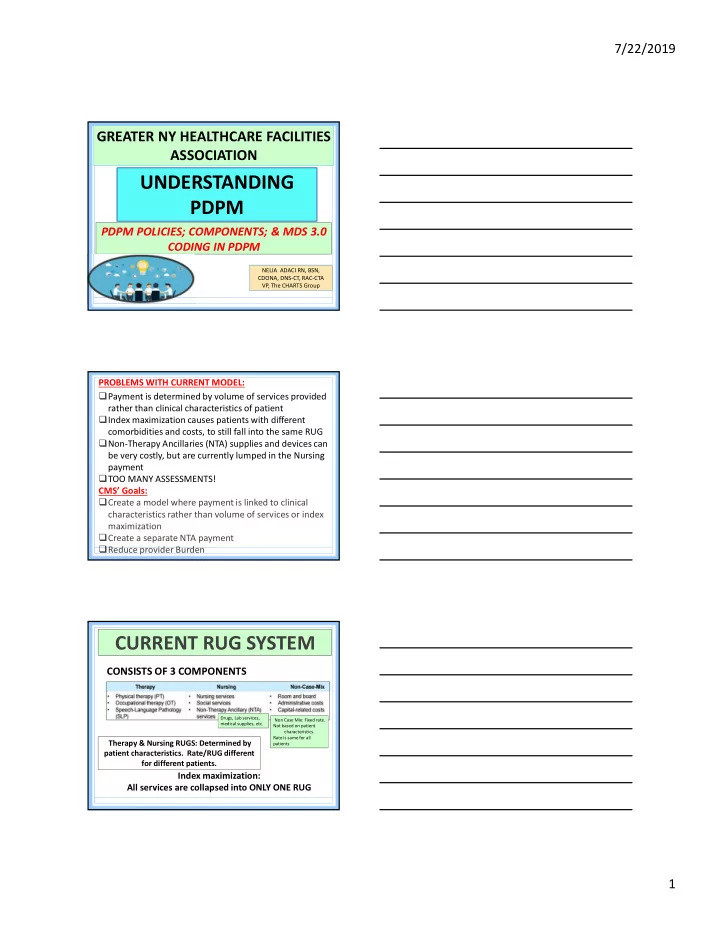
CURRENT RUG SYSTEM
CONSISTS OF 3 COMPONENTS
Therapy & Nursing RUGS: Determined by patient characteristics. Rate/RUG different for different patients.
Drugs, Lab services, medical supplies, etc. Non Case Mix: Fixed rate. Not based on patient characteristics. Rate is same for all patients
Index maximization: All services are collapsed into ONLY ONE RUG