
6/20/2019 1
47th Annual UCSF Advances in Internal Medicine
VENOUS THROMBOEMBOLISM: So Many Questions…Oy!
Andrew D. Leavitt, MD
June 20, 2019
Topic Outline
1. Direct Oral Anti-Coagulants (DOACs): A Little Review 2. Obesity 3. Gastric Bypass 4. Coagulation Tests and Drug levels 5. Superficial Venous Thrombosis (SVT) 6. IVC Filters 7. Flight / Extended Travel 8. Your Cases
- A 32 year old man comes to your office with 5 days of
progressive discomfort in his left leg, and 2 days of swelling from the knee down.
- No significant PMH. He takes no Rx. He cannot recall any
particular injury. He is afebrile.
- History and exam lead you to suspect a DVT. You send him
for a left leg ultrasound
CASE 1: What Would You Do?
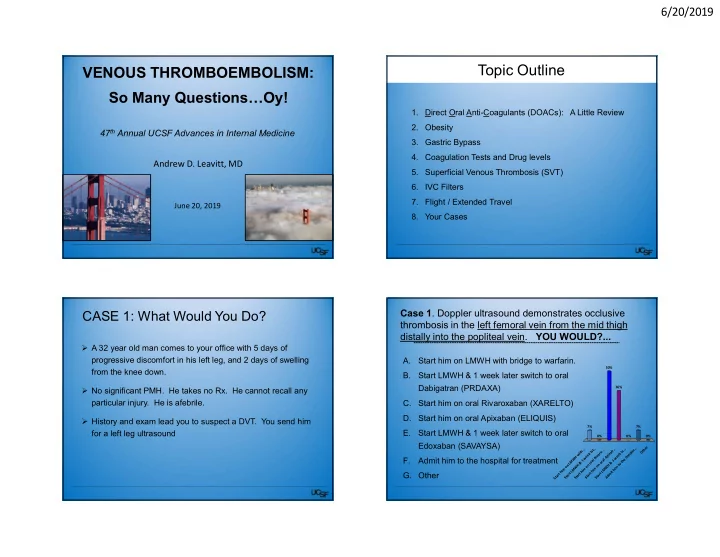
Case 1. Doppler ultrasound demonstrates occlusive thrombosis in the left femoral vein from the mid thigh distally into the popliteal vein. YOU WOULD?...
A. Start him on LMWH with bridge to warfarin. B. Start LMWH & 1 week later switch to oral Dabigatran (PRDAXA) C. Start him on oral Rivaroxaban (XARELTO) D. Start him on oral Apixaban (ELIQUIS) E. Start LMWH & 1 week later switch to oral Edoxaban (SAVAYSA) F. Admit him to the hospital for treatment
- G. Other
S t a r t h i m
- n
L M W H w i t h . . . S t a r t L M W H & 1 w e e k l a t . . S t a r t h i m
- n
- r
a l R i v a r
- .
. . S t a r t h i m
- n
- r
a l A p i x a b . . S t a r t L M W H & 1 w e e k l a . . . A d m i t h i m t
- t
h e h
- s
p i t a . . . O t h e r 7% 0% 50% 0% 7% 0% 36%