
SLIDE 1
Steps to stratified medicine: an example from lung cancer
Kinga Malottki k.malottki@bham.ac.uk
Using a treatment
Xinghua Hu S, Foster T, Kieffaber A. Pharmacogenomics and personalized medicine: mapping future value creation. BioTechniques 2005; 39 (4)
r e s p
- n
d e r s n
- n
‐ r e s p
- n
d e r s toxicity
Using a treatment – predictive biomarkers
r e s p
- n
d e r s n
- n
‐ r e s p
- n
d e r s
Biomarker 1 Biomarker 2 BM 3
toxicity
Erlotinib for Non‐Small‐Cell Lung Cancer (NSCLC)
- Population: patients with NSCLC after or unsuitable
for chemotherapy
- Intervention: erlotinib at any dose
- Comparator: any, including no
- Outcomes: overall survival, response
- Design: any, except case reports
- Biomarkers: EGFR expression, EGFR copy number,
EGFR mutation, KRAS mutation
Erlotinib for NSCLC
- Not a systematic review
- Search in MEDLINE up to March 2010
- Internet searches
- Checking references of included studies
- 10 completed studies (1 RCT: BR.21)
- 2 ongoing RCTs (MARVEL, SATURN)
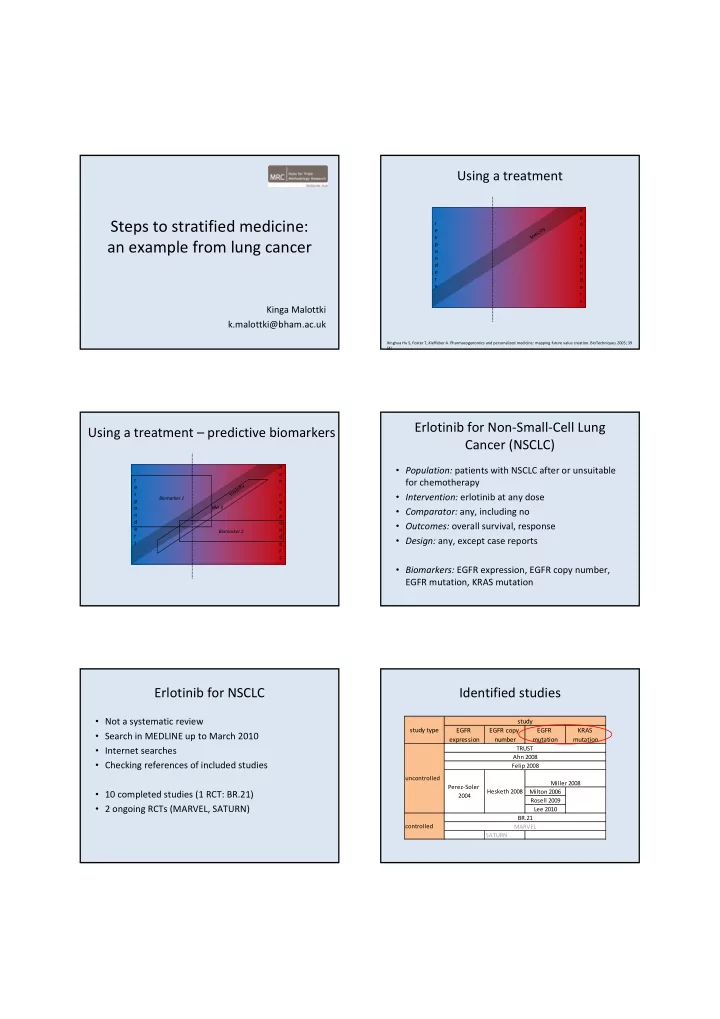
Identified studies
EGFR expression EGFR copy number EGFR mutation KRAS mutation Milton 2006 Rosell 2009 Lee 2010 SATURN uncontrolled controlled study type Perez‐Soler 2004 Hesketh 2008 TRUST BR.21 MARVEL study Miller 2008 Felip 2008 Ahn 2008