
SLIDE 1
1
Dr ASHOK V CHORDIYA
Director Fortis Hospital Noida
LEARNINGS OF A HOSPITAL CLINICIAN ADMINISTRATOR
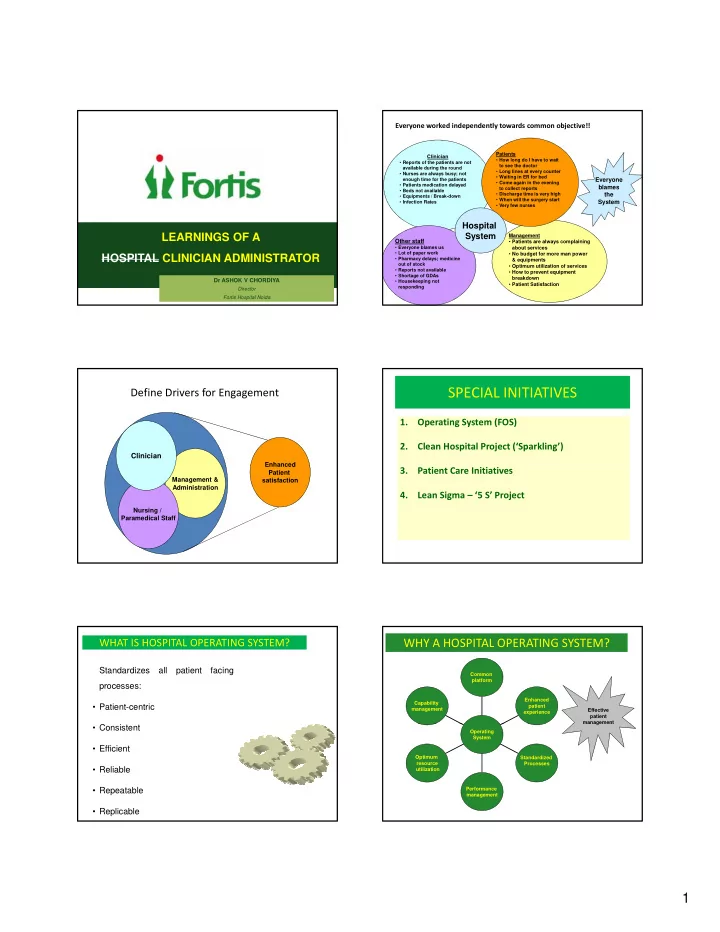
Everyone blames the System
Everyone worked independently towards common objective!!
Clinician
- Reports of the patients are not
available during the round
- Nurses are always busy; not
enough time for the patients
- Patients medication delayed
- Beds not available
- Equipments / Break-down
- Infection Rates
Patients
- How long do I have to wait
to see the doctor
- Long lines at every counter
- Waiting in ER for bed
- Come again in the evening
to collect reports
- Discharge time is very high
- When will the surgery start
- Very few nurses
Management
- Patients are always complaining
about services
- No budget for more man power
& equipments
- Optimum utilization of services
- How to prevent equipment
breakdown
- Patient Satisfaction
y
Other staff
- Everyone blames us
- Lot of paper work
- Pharmacy delays; medicine
- ut of stock
- Reports not available
- Shortage of GDAs
- Housekeeping not
responding
Hospital System
Define Drivers for Engagement
Enhanced
Clinician
Management & Administration Enhanced Patient satisfaction Nursing / Paramedical Staff
SPECIAL INITIATIVES
1. Operating System (FOS) 2. Clean Hospital Project (‘Sparkling’) 3. Patient Care Initiatives 4. Lean Sigma – ‘5 S’ Project
WHAT IS HOSPITAL OPERATING SYSTEM?
Standardizes all patient facing processes:
- Patient-centric
- Consistent
- Efficient
- Reliable
- Repeatable
- Replicable
Effective patient management
WHY A HOSPITAL OPERATING SYSTEM?
Capability management Enhanced patient experience Common platform management Optimum resource utilization Performance management Standardized Processes Operating System