
SLIDE 1
William M. Gilbert, MD Regional Medical Director, Sutter Health & Clinical Professor Department of OB/GYN University of California, Davis Speaker honorarium - Lumara Health No conflicts with respect to this lecture A.
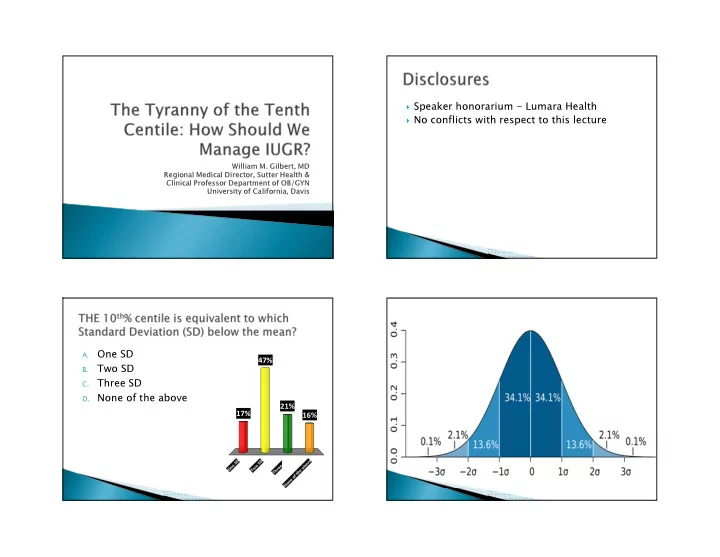
One SD
B.
Two SD
C.
Three SD
- D. None of the above